
How to Reconstitute Peptides: Step-by-Step Dosing Guide (2026)

How Do You Reconstitute a Peptide?
Add bacteriostatic water slowly down the inner glass wall of the lyophilised vial, never directly onto the powder. Standard example: 2mL BAC water into a 5mg vial yields 2500mcg/mL. A 250mcg dose draws as 0.10mL (10 units on a U-100 syringe). Swirl gently, label, refrigerate.
Reconstitution is the step that ends peptide protocols before they start. Add water directly onto the powder and you risk fragmenting peptide chains. Get the maths wrong and you inject ten times your intended dose. Use the wrong diluent and you contaminate the entire vial before drawing a single unit.
Most guides skip straight to dosing. This one starts where the work actually begins: technique, maths, storage, and the mistakes that cost researchers weeks of progress.
Use our peptide reconstitution calculator to skip the manual maths once you have read through the technique below.
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice.
Why Reconstitution Technique Matters: The Science
Lyophilised peptides are freeze-dried under vacuum to maximise shelf stability. The reconstitution step rehydrates the powder into a uniform solution. Done correctly, the peptide resumes its native conformation. Done incorrectly, aggregation, fragmentation, or microbial contamination can render the compound inactive or unsafe.
Peptides are short chains of amino acids held together by peptide bonds. In solution, those bonds are vulnerable to hydrolysis, oxidation, and physical shear forces. The seminal review by Manning et al. (2010) in Pharmaceutical Research established that protein and peptide pharmaceuticals in aqueous solution degrade through predictable chemical pathways -- hydrolysis, deamidation, oxidation -- that accelerate with heat, light, and agitation.
When you inject water directly onto a lyophilised peptide cake under pressure, you create localised mechanical shear at the point of impact. Bekard et al. (2011) demonstrated in Biopolymers that shear flow induces conformational changes in protein structure, promoting nonnative intermolecular contacts. At peptide scale this translates to partial unfolding and the formation of aggregates that are biologically inert at best and immunogenic at worst.
The aggregation risk is compounded by surface tension effects. in Pharmaceutical Research showed that air-water interfaces are primary nucleation sites for protein aggregation -- the reason experienced researchers add water down the glass wall rather than through air directly onto powder. Directing water along the vial wall eliminates the air-water impact and allows the powder to dissolve by capillary action rather than brute hydration.
Understanding this mechanism is not academic pedantry. If you are researching compounds such as BPC-157 or TB-500 for tissue recovery models, the biological activity of the compound depends entirely on the integrity of its primary structure at the point of administration. A poorly reconstituted vial is an expensive control group experiment, not a research run.
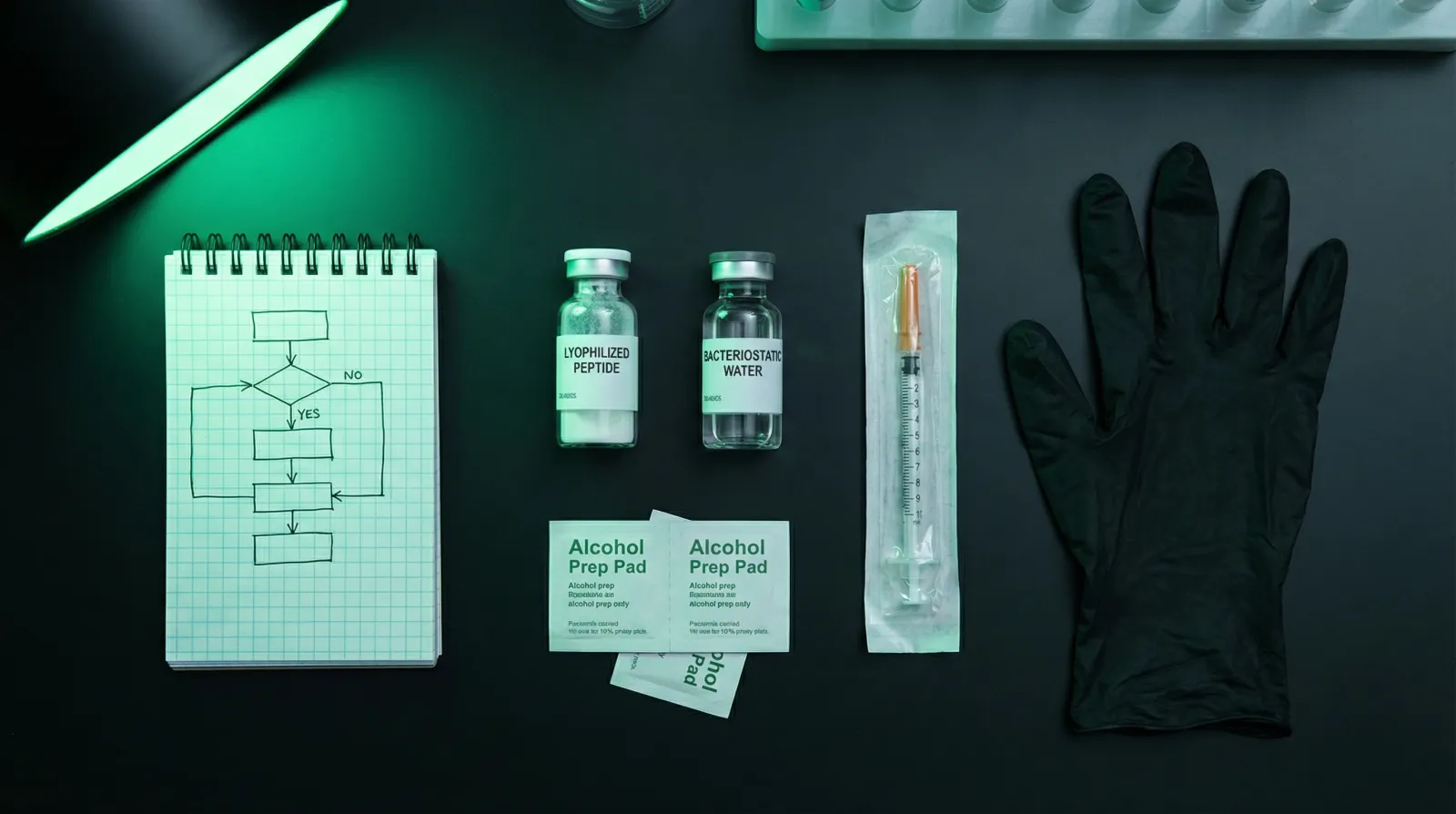
Supplies Checklist
Five supplies are non-negotiable: a lyophilised peptide vial, bacteriostatic water, a U-100 insulin syringe (29-31 gauge), alcohol swabs, and a sharps bin. Pull everything from one trusted research-grade supplier where possible to keep batch quality consistent. Substituting sterile water for bacteriostatic water in a multi-draw vial is the single most common sourcing mistake.
| Item | Spec | Where to get | Why it matters |
|---|---|---|---|
| Lyophilised peptide vial | 2mg, 5mg, or 10mg, freeze-dried, sealed | Research peptide supplier with per-batch CoA | Quality and identity are only verifiable through a third-party Certificate of Analysis |
| Bacteriostatic water (BAC water) | 0.9% benzyl alcohol preservative, 30mL multi-dose vial | Pharmacy or research peptide supplier | Allows multi-draw use for up to 28 days; sterile water and saline are not substitutes for multi-dose protocols |
| U-100 insulin syringe | 29-31 gauge, 0.5mL or 1mL barrel, fixed needle | Pharmacy | 1 unit = 0.01mL; precision needed for sub-0.1mL draws common in peptide research |
| Alcohol swabs | 70% isopropyl alcohol, individually wrapped | Pharmacy | Required before every needle insertion into the vial septum to prevent microbial contamination |
| Sharps bin | FDA-cleared puncture-resistant container | Pharmacy | Used syringes must never be recapped or placed in household waste |
| Marker or label tape | Waterproof, permanent ink | Stationery | Label every vial with compound name, concentration, date reconstituted, and expiry |
Diluent Comparison: Bacteriostatic Water vs Sterile Water vs Saline
Choosing the wrong diluent is the most common mistake beginners make. The three options available are not interchangeable. They differ in preservative content, permitted use duration, and compatibility with specific peptide classes.
| Diluent | Preservative | Multi-dose safe? | In-use shelf life (refrigerated) | Best used for | Avoid when |
|---|---|---|---|---|---|
| Bacteriostatic water (BAC water) | 0.9% benzyl alcohol | Yes | Up to 28 days after opening | Most peptides requiring multiple draws over days or weeks | Peptides with known benzyl alcohol sensitivity; neonatal use |
| Sterile water for injection | None | No (single use only) | Use immediately; discard remainder | Single-dose reconstitution; peptides sensitive to benzyl alcohol | Any multi-draw protocol (contamination risk after first draw) |
| Normal saline (0.9% NaCl) | None (usually) | No | Use immediately; discard remainder | Some lyophilised pharmaceuticals formulated for saline reconstitution | General research peptide reconstitution; may affect solubility of some peptides |
| Acetic acid (0.1-1% solution) | None | No | Use immediately | Poorly soluble peptides (e.g. certain growth hormone fragments) | Standard water-soluble peptides; can cause injection site irritation if used undiluted |
For the vast majority of research peptides -- BPC-157, TB-500, CJC-1295, Ipamorelin, Selank, Semax, Thymosin Alpha-1 -- bacteriostatic water is the correct default diluent. It provides a sterile, preserved environment that allows multiple draws from a single reconstituted vial over a standard research block. If you are running a CJC-1295 and Ipamorelin protocol with twice-daily administrations, BAC water is not optional; it is structural to the protocol's safety.
Step-by-Step Reconstitution Protocol
The full protocol has eight discrete steps. Skipping any of them -- even the seemingly minor ones like swabbing the septum before every draw -- introduces compounding contamination or dosing risks. Follow this sequence for every vial you reconstitute, regardless of compound or concentration.
- Prepare your workspace. Use a clean, hard, flat surface. A fresh paper towel or disposable bench liner is sufficient for research use. Do not work over carpet or upholstered surfaces. Wash hands with soap and water for at least 20 seconds. If gloves are available, use them.
- Gather all supplies before opening anything. Have the peptide vial, BAC water vial, insulin syringe(s), alcohol swabs, sharps bin, and labels on the bench before you break any seals. Interrupting the process to retrieve a forgotten item introduces contamination risk.
- Inspect the peptide vial. Check for: intact rubber septum with no visible puncture history, secure crimped aluminium collar, clearly visible lyophilised cake (white or off-white powder or porous solid, not discoloured, not liquefied). Any vial that appears pre-dissolved, discoloured, or has a compromised seal should be discarded.
- Swab both vial tops. Using separate alcohol swabs, wipe the rubber septum of the peptide vial and the rubber septum of the BAC water vial. Allow to air-dry for 10-15 seconds. Do not blow on them; the moisture from breath introduces contaminants. This step is repeated before every needle insertion into any vial.
- Draw the calculated volume of BAC water. Insert the syringe needle through the BAC water septum at a 45-degree angle, draw back the plunger slowly to your target volume (see dosing maths section below), then withdraw. Check the syringe barrel for air bubbles; if present, invert the syringe and tap gently, then depress slowly to expel before proceeding.
- Add water to the peptide vial down the inner glass wall. Insert the needle through the peptide vial septum and position the needle tip so it touches the inner glass wall of the vial at an angle. Depress the plunger slowly and steadily, allowing the water to run down the glass wall and dissolve the powder by gravity and capillary action. This is the most critical technical step. Never inject water directly onto the lyophilised cake.
- Swirl, do not shake. Once all the water is added, gently rotate the vial between your fingers in a slow rolling motion for 20-30 seconds. The cake typically dissolves in under 60 seconds if the water was added correctly. If dissolution is slow, allow the vial to sit at room temperature for 2-3 minutes and swirl again. A clear, particle-free solution is the target appearance. If you see persistent cloudiness or visible particulate matter, the vial may be degraded or contaminated; do not use.
- Label immediately and refrigerate. Before you set the vial down, label it with: compound name, total peptide mass (e.g. 5mg), volume of BAC water added (e.g. 2mL), resulting concentration (e.g. 2500mcg/mL), date reconstituted, and calculated expiry date (28 days from today for BAC water reconstitution). Store at 2-8 degrees Celsius in the back of the refrigerator, away from the light seal. Do not freeze a reconstituted peptide.
Dosing Maths: The Concentration Formula and Worked Examples
The core formula is: Dose (mcg) divided by Concentration (mcg/mL) equals Volume to draw (mL). Multiply mL by 100 to get insulin syringe units. Every dosing error in peptide research traces back to a failure to complete this calculation before drawing. Work through it on paper before touching a syringe.
The formula:
Volume to draw (mL) = Target dose (mcg) / Concentration (mcg/mL)
Concentration is set by you at reconstitution:
Concentration (mcg/mL) = Total peptide mass (mcg) / Volume of BAC water added (mL)
Note: 1mg = 1000mcg. A 5mg vial contains 5000mcg total.
| Vial Size | BAC Water Added | Resulting Concentration | 250mcg Dose Draws As | 500mcg Dose Draws As | 1000mcg Dose Draws As |
|---|---|---|---|---|---|
| 2mg (2000mcg) | 1mL | 2000mcg/mL | 0.125mL (12.5 units) | 0.25mL (25 units) | 0.50mL (50 units) |
| 2mg (2000mcg) | 2mL | 1000mcg/mL | 0.25mL (25 units) | 0.50mL (50 units) | 1.00mL (100 units) |
| 5mg (5000mcg) | 1mL | 5000mcg/mL | 0.05mL (5 units) | 0.10mL (10 units) | 0.20mL (20 units) |
| 5mg (5000mcg) | 2mL | 2500mcg/mL | 0.10mL (10 units) | 0.20mL (20 units) | 0.40mL (40 units) |
| 5mg (5000mcg) | 5mL | 1000mcg/mL | 0.25mL (25 units) | 0.50mL (50 units) | 1.00mL (100 units) |
| 10mg (10000mcg) | 2mL | 5000mcg/mL | 0.05mL (5 units) | 0.10mL (10 units) | 0.20mL (20 units) |
| 10mg (10000mcg) | 5mL | 2000mcg/mL | 0.125mL (12.5 units) | 0.25mL (25 units) | 0.50mL (50 units) |
| 10mg (10000mcg) | 10mL | 1000mcg/mL | 0.25mL (25 units) | 0.50mL (50 units) | 1.00mL (100 units) |
Practical concentration selection principle: Choose a BAC water volume that results in a draw volume of at least 0.05mL (5 units) for your target dose. Draws smaller than 5 units are imprecise with standard U-100 syringes and introduce meaningful dosing variance. If your target dose is 250mcg from a 5mg vial, adding 2mL of BAC water (yielding a 10-unit draw) is preferable to adding 1mL (yielding a 5-unit draw that sits at the edge of measurement precision).
Worked Example: BPC-157 at 250mcg twice daily
- Vial: 5mg BPC-157 (5000mcg total)
- BAC water added: 2mL
- Concentration: 5000 / 2 = 2500mcg/mL
- Volume per 250mcg dose: 250 / 2500 = 0.10mL = 10 units on U-100 syringe
- Doses per vial at 250mcg: 5000 / 250 = 20 doses
- Duration: 20 doses at twice daily = 10 days per vial
- Protocol duration of 12 weeks (84 days, 168 doses): approximately 8.4 vials required
Running a full injury recovery research block using BPC-157 alongside TB-500? See our BPC-157 and TB-500 post-surgery recovery protocol for compound-specific dosing and sequencing detail.
Worked Example: CJC-1295 at 100mcg per injection
- Vial: 2mg CJC-1295 (2000mcg total)
- BAC water added: 2mL
- Concentration: 2000 / 2 = 1000mcg/mL
- Volume per 100mcg dose: 100 / 1000 = 0.10mL = 10 units on U-100 syringe
- Doses per vial: 2000 / 100 = 20 doses
For full protocol detail on growth hormone secretagogues see our CJC-1295 complete guide and the combined CJC-1295 and Ipamorelin guide.
Subcutaneous Injection Technique
Subcutaneous (SubQ) injection deposits the solution into the fatty tissue layer just beneath the skin. For research purposes, SubQ is the standard route for most peptides because the tissue is highly vascularised, absorption is reliable and consistent, and the technique carries lower risk than intramuscular injection when performed correctly.
Injection site selection:
The three most practical SubQ sites are the abdomen (2-3cm from the navel), the upper thigh (lateral aspect, midpoint), and the upper outer arm. Rotate sites with every injection to prevent lipodystrophy -- localised fat tissue breakdown from repeated injection at the same point. If administering twice daily, use opposite sides of the abdomen or alternate between abdomen and thigh.
Injection technique:
- Swab the injection site with an alcohol swab. Allow to dry completely (10-15 seconds). Injecting through wet alcohol stings and carries trace alcohol into the SubQ layer.
- Pinch a small fold of skin between thumb and forefinger -- about 2-3cm of tissue. This lifts the SubQ layer away from underlying muscle.
- Hold the syringe at 45 degrees for thin individuals or 90 degrees for those with more SubQ tissue. Insert the needle in one smooth, confident motion.
- Release the skin pinch. Draw back the plunger slightly (aspiration). If blood enters the barrel, you have hit a vessel. Withdraw without injecting, apply gentle pressure, use a fresh syringe and new site.
- Inject slowly and steadily. A 0.10mL volume should take approximately 5-10 seconds. Rapid injection increases local discomfort and can cause a localised weal.
- Withdraw the needle at the same angle it entered. Apply gentle pressure with a clean swab for 10 seconds. Do not rub; rubbing disperses the compound into a wider area and can cause bruising.
- Dispose of the syringe immediately in your sharps bin. Never recap a used needle.
On injection site pain: Mild burning or stinging at the injection site is common and typically resolves within a minute. It is more common with higher-concentration solutions and with BAC water that has a higher benzyl alcohol content relative to the injection volume. If you routinely experience significant site pain, try reducing concentration by adding more BAC water (which increases draw volume but dilutes the benzyl alcohol per mL), or allow the reconstituted vial to reach room temperature before drawing -- injecting cold solution from the refrigerator is a common cause of unnecessary discomfort.
Storage, Shelf Life, and Stability
Lyophilised (unreconstituted) peptides stored correctly in a sealed vial at 2-8 degrees Celsius are stable for 12-24 months from manufacture date. Once reconstituted in bacteriostatic water, shelf life drops to approximately 28 days refrigerated. These are not approximate guidelines; they reflect the degradation kinetics of peptide bonds in aqueous solution under typical storage conditions.
| State | Storage Temp | Light exposure | Shelf life | Notes |
|---|---|---|---|---|
| Lyophilised, sealed vial | 2-8°C (refrigerator) | Away from light | 12-24 months | Many peptides tolerate ambient shipping for up to 5-7 days without meaningful degradation |
| Lyophilised, sealed vial (long term) | -20°C (freezer) | Away from light | 2-5 years | Do not freeze-thaw repeatedly; each cycle introduces aggregation risk |
| Reconstituted in BAC water | 2-8°C (refrigerator) | Away from light | Up to 28 days | Label with expiry date at time of reconstitution; discard at 28 days regardless of remaining volume |
| Reconstituted in sterile water | 2-8°C (refrigerator) | Away from light | Single use (24 hrs max) | No preservative; discard remaining volume after first draw |
| Reconstituted, left at room temperature | 15-25°C | Any | 4-8 hours maximum | Heat and UV accelerate hydrolysis and oxidation; return vial to refrigerator within minutes of each draw |
| Reconstituted, frozen | -20°C | Away from light | Not recommended | Freeze-thaw cycles accelerate aggregation in solution; lyophilise-freeze then reconstitute fresh instead |
The underlying degradation science: Manning et al. (2010) documented that the primary aqueous degradation pathways for peptides include deamidation of asparagine and glutamine residues and oxidation of methionine, tryptophan, and cysteine residues. Both pathways are temperature-dependent and follow Arrhenius kinetics -- meaning even small increases in storage temperature have disproportionate effects on degradation rate. This is the biochemical basis for the strict 2-8 degree Celsius recommendation; it is not arbitrary.
Common Mistakes and How to Avoid Them
These are the seven errors that account for the majority of failed research outcomes, contaminated vials, and dosing errors in peptide research settings:
| Mistake | What it causes | How to avoid it |
|---|---|---|
| Injecting BAC water directly onto the powder | Peptide fragmentation through mechanical shear; aggregation at the impact site; reduced biological activity | Always direct water down the inner glass wall of the vial at an angle |
| Shaking instead of swirling | Air-water interface agitation accelerates aggregation; produces foam that traps compound and is difficult to draw | Roll gently between fingers or swirl in slow circles only |
| Using sterile water for a multi-draw vial | Microbial contamination after first septum puncture; no preservative to arrest bacterial growth | Use bacteriostatic water for any vial that will be drawn from more than once |
| Not swabbing the septum before each draw | Introduction of skin flora (Staphylococcus epidermidis common) into the vial; cumulative contamination across draws | New alcohol swab, allow to dry, before every needle insertion |
| Incorrect concentration maths (most dangerous error) | 10x overdose (injecting 0.10mL from a 10mg/mL vial thinking it is 1mg/mL) or gross underdose; neither has a safe correction mid-injection | Write out the full calculation before drawing; double-check on a calculator; cross-reference against a reference table before every new vial |
| Storing reconstituted vials in the refrigerator door | Temperature cycling from door opening; accelerated degradation; shortened effective shelf life | Store at the back of the main fridge compartment where temperature is most stable |
| Drawing air bubbles into the syringe | Not dangerous (SubQ air is absorbed rapidly) but reduces dose accuracy by displacing solution volume | Invert syringe, tap to collect bubbles at needle end, depress slowly to expel before injecting |
Where to source it
The hard part with research peptides isn't the protocol. It's finding a supplier that can prove what's in the vial. We assessed dozens against per-batch, third-party testing. A handful passed.
See the sources that passed →Sourcing and Verifying Research Peptides
The quality of reconstitution technique is irrelevant if the compound in the vial is not what the label claims. Third-party analytical verification -- specifically high-performance liquid chromatography (HPLC) for purity and mass spectrometry (MS) for identity -- is the only way to confirm a research peptide is correctly identified and free from common adulterants. A Certificate of Analysis (CoA) without the testing laboratory's name, HPLC trace, and date is not a CoA; it is a label.
What to look for in a supplier's Certificate of Analysis:
- Testing performed by a named, independent third-party laboratory (not the manufacturer's in-house lab)
- HPLC purity result expressed as a percentage (research-grade threshold: ≥98% purity)
- Mass spectrometry identity confirmation with expected vs observed molecular weight listed
- Batch or lot number on the CoA matching the batch number on the vial label
- Test date (CoA older than 18 months on a new-stock vial is a red flag)
- Endotoxin testing result (LAL test; expressed in EU/mg; should be below 2 EU/mg for injectable research use)
The regulatory landscape for research peptides shifted significantly in 2024-2025 following the FDA's compounding policy updates. Understanding the current framework helps research buyers make informed sourcing decisions. See our detailed breakdown of what the FDA reclassification means for peptide research and the update on which peptides are available again in 2026.
Suppliers worth considering for bacteriostatic water, insulin syringes, and quality peptide vials for research purposes:
Share this article
Frequently Asked Questions
How much bacteriostatic water do I add to a 5mg peptide vial?
Can I use sterile water instead of bacteriostatic water to reconstitute peptides?
How do I calculate units on an insulin syringe for my peptide dose?
How long does a reconstituted peptide vial last in the fridge?
What does a properly reconstituted peptide look like?
Is it safe to inject bacteriostatic water and what is the benzyl alcohol risk?
Read Next


Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.