
7 Best Peptides for Injury Recovery (2026 Guide)

The 7 Most Effective Peptides for Injury Recovery in 2026
The best peptides for injury recovery are BPC-157, TB-500, the Wolverine Stack (BPC-157 + TB-500 combined), GHK-Cu, CJC-1295 with Ipamorelin, Thymosin Alpha-1, and KPV. Each targets a different aspect of the healing process, from localised tissue repair to systemic inflammation control, and the right choice depends on the type of injury, its severity, and where you are in the recovery timeline.
Peptide therapy for injuries has shifted from fringe biohacking to a legitimate medical conversation. With the FDA's 2026 reclassification restoring legal access to several key compounds through compounding pharmacies, clinicians and patients now have options that were effectively unavailable for years. This guide ranks the seven peptides with the strongest evidence and practical track record for injury recovery, explains what each one does, and helps you determine which ones match your situation.
1. BPC-157: The Gold Standard for Localised Tissue Repair
BPC-157 (Body Protection Compound-157) is the single most effective peptide for targeted injury recovery, particularly for tendons, ligaments, muscles, and the gastrointestinal tract. It works by upregulating growth factor expression, stimulating angiogenesis (new blood vessel formation), and modulating nitric oxide pathways to accelerate tissue repair at the injection site.
What makes BPC-157 exceptional is its versatility. Research published in the Journal of Physiology demonstrates its efficacy across tendon transections, muscle crush injuries, ligament tears, and even bone fractures in animal models (Kang et al. 2018). The mechanism is not a single pathway but a coordinated upregulation of VEGF, FGF, and other growth factors that collectively accelerate the body's natural repair process.
For practical use, BPC-157 is typically administered subcutaneously near the injury site at 250-500mcg once or twice daily. A standard protocol runs 4-6 weeks. Injection close to the injury matters because BPC-157's effects are most pronounced locally, though systemic benefits have been documented as well. Our BPC-157 dosing protocol guide covers loading and maintenance phases in detail.
One decision you will face is delivery method. BPC-157 is available in both injectable and oral forms, and the choice depends on injury location. Injectable is superior for musculoskeletal injuries (shoulders, knees, elbows), while oral BPC-157 targets the GI tract more effectively. The tradeoffs are covered in our oral vs injectable comparison.
Best for: Tendon injuries, ligament tears, muscle strains, post-surgical recovery, rotator cuff injuries, Achilles tendon issues, and joint pain.
2. TB-500: Systemic Healing and Mobility Restoration
TB-500 (Thymosin Beta-4) is the best peptide for systemic injury recovery, meaning injuries that affect multiple areas or require whole-body healing support. Unlike BPC-157's localised action, TB-500 circulates systemically after injection and upregulates actin, a protein essential for cell migration, blood vessel growth, and tissue repair throughout the body.
The key mechanism is TB-500's ability to promote cell migration to injury sites. When tissue is damaged, repair depends on immune cells and fibroblasts reaching the area quickly. TB-500 facilitates this by modulating actin polymerisation, effectively giving your repair cells better mobility. Research in Annals of the New York Academy of Sciences has documented its role in wound healing, cardiac repair, and reducing inflammation.
The standard TB-500 dosage protocol uses a loading phase of 5-10mg per week (split into 2-3 injections) for 4-6 weeks, followed by a maintenance phase of 2-5mg per week. Unlike BPC-157, injection site is less critical because TB-500 works systemically. Subcutaneous injection in the abdomen is the most common approach.
TB-500 also has documented benefits for reducing scar tissue formation and improving flexibility in damaged tissue, which matters for athletes and anyone recovering from surgery. Our TB-500 complete guide covers the full evidence base, and the side effects profile is important reading before starting any protocol.
Best for: Multi-site injuries, post-surgical recovery requiring systemic healing, chronic inflammatory conditions, athletic recovery from overtraining, and injuries where mobility and flexibility restoration are priorities.
3. The Wolverine Stack: BPC-157 + TB-500 Combined
The Wolverine Stack is the combination of BPC-157 and TB-500 run simultaneously, and it is the most potent peptide recovery protocol available. The name is not subtle, but the logic is sound: BPC-157 handles targeted repair at the injury site while TB-500 supports systemic healing, cell migration, and inflammation control. Together, they cover both local and global aspects of recovery.
This is not just theory. The two peptides work through complementary mechanisms. BPC-157 upregulates local growth factors (VEGF, FGF, EGF) and promotes angiogenesis at the injury site. TB-500 enhances cell migration systemically and reduces fibrosis. Running them together means the body receives localised repair signals and systemic healing support simultaneously, which neither peptide delivers alone.
The standard Wolverine Stack protocol pairs BPC-157 at 250-500mcg daily (injected near the injury) with TB-500 at 5-10mg per week (split into 2-3 subcutaneous injections). Most practitioners run the stack for 6-8 weeks. Our dedicated Wolverine Stack protocol guide covers timing, injection technique, and cycling in full detail. For a side-by-side breakdown of how these two peptides differ and complement each other, see our BPC-157 vs TB-500 comparison.
The Wolverine Stack is the go-to recommendation for serious injuries: ACL reconstructions, rotator cuff repairs, Achilles ruptures, and any recovery where downtime needs to be minimised. It is also the most commonly prescribed peptide protocol in sports medicine clinics that offer peptide therapy.
Best for: Serious injuries requiring maximum recovery support, post-surgical rehabilitation, ACL/MCL repairs, rotator cuff surgery, and anyone who wants the most aggressive peptide recovery protocol available.
4. GHK-Cu: Wound Healing, Collagen, and Tissue Remodelling
GHK-Cu (glycyl-L-histidyl-L-lysine copper complex) is a naturally occurring copper peptide that declines significantly with age and plays a central role in wound healing, collagen synthesis, and tissue remodelling. For injury recovery, GHK-Cu excels in the later stages of healing where tissue quality and scar remodelling matter most.
The mechanism is multifaceted. GHK-Cu activates wound repair genes, stimulates collagen and elastin production, attracts immune cells to injury sites, and has potent anti-inflammatory properties. Research published in the Journal of Biological Chemistry has shown it can reset gene expression patterns in damaged tissue toward a healthier repair state (Benschop et al. 2014). Crucially, it also inhibits the formation of excessive scar tissue, which distinguishes it from peptides that primarily accelerate the initial healing phase.
GHK-Cu is unique among recovery peptides because it works both topically and by injection. Topical copper peptide serums support skin wound healing, surgical incision recovery, and surface-level tissue repair. Injectable GHK-Cu targets deeper tissue remodelling, making it relevant for joint injuries, surgical recovery, and chronic tissue degradation.
A typical injectable protocol runs 1-2mg daily for 4-8 weeks. Topical application is simpler and can continue indefinitely. GHK-Cu pairs well with BPC-157 (BPC-157 accelerates initial repair, GHK-Cu improves the quality of healed tissue) and is increasingly prescribed alongside the Wolverine Stack for comprehensive recovery protocols.
Best for: Post-surgical scar management, wound healing, collagen-dependent recovery (skin, tendons, ligaments), chronic tissue degeneration, and injuries where tissue quality and long-term remodelling outcomes matter as much as healing speed.
5. CJC-1295 + Ipamorelin: Growth Hormone for Recovery
CJC-1295 combined with Ipamorelin is the most widely prescribed growth hormone secretagogue stack, and its relevance to injury recovery lies in one fundamental fact: growth hormone is the master regulator of tissue repair. By stimulating the body's own GH production, this stack elevates IGF-1 levels, which directly accelerates muscle repair, bone healing, tendon strengthening, and recovery from surgery.
CJC-1295 is a growth hormone releasing hormone (GHRH) analogue that extends the natural GH pulse. Ipamorelin is a selective growth hormone secretagogue that triggers GH release without the appetite-stimulating and cortisol-raising side effects of older secretagogues like GHRP-6. Together, they produce a synergistic GH elevation that is cleaner and more sustained than either peptide alone.
For injury recovery specifically, the elevated IGF-1 from this stack supports protein synthesis in damaged muscle, accelerates collagen production for connective tissue repair, and enhances bone mineral density during fracture healing. Research on GH's role in recovery is well established in clinical literature, and the CJC-1295/Ipamorelin combination is the preferred method of elevating GH without exogenous hormone injection.
The standard protocol is 100mcg CJC-1295 (no DAC) combined with 100-200mcg Ipamorelin, administered subcutaneously before bed, 5 nights per week. The bedtime dosing aligns with the body's natural GH pulse during deep sleep. Most recovery-focused protocols run 8-12 weeks. This stack is particularly valuable for older patients (over 40) where natural GH levels have already declined significantly. Our best peptides for men over 40 guide covers this age-related context in detail.
Best for: Slow-healing injuries in patients over 35, fracture recovery, muscle wasting after immobilisation, post-surgical recovery where lean mass preservation matters, and as an adjunct to BPC-157/TB-500 protocols for accelerated results.
6. Thymosin Alpha-1: Immune Support During Recovery
Thymosin Alpha-1 is an immune-modulating peptide that supports injury recovery through a different pathway than the tissue-repair peptides above. Its primary role is optimising immune function during the healing process, which matters because the immune system orchestrates the entire inflammatory and repair cascade after injury.
When tissue is damaged, the immune system must execute a precise sequence: initial inflammation to clear debris, recruitment of repair cells, tissue remodelling, and resolution of inflammation. If immune function is compromised (from stress, age, poor sleep, or overtraining), this sequence stalls or becomes dysregulated. Thymosin Alpha-1 modulates T-cell function and dendritic cell maturation to keep the immune repair cascade on track.
This peptide is already an approved pharmaceutical in over 35 countries under the brand name Zadaxin, primarily for hepatitis and as a cancer immunotherapy adjunct. Its safety profile is among the best-established of any therapeutic peptide. For injury recovery, it is most valuable when the patient is immunocompromised, under high stress, recovering from illness alongside an injury, or dealing with chronic wounds that are not healing on expected timelines.
The standard dosage is 1.6mg subcutaneously, 2-3 times per week. It stacks cleanly with BPC-157 and TB-500 without interaction concerns. Thymosin Alpha-1 is not a first-line recovery peptide for a simple muscle strain, but it becomes highly relevant for complex recoveries, post-surgical patients at infection risk, and older individuals whose immune function may be limiting their healing rate.
Best for: Complex recoveries with infection risk, post-surgical immune support, chronic non-healing wounds, recovery in immunocompromised or stressed patients, and as an adjunct in multi-peptide recovery protocols for comprehensive support.
7. KPV: Anti-Inflammatory Peptide for Recovery
KPV is a tripeptide fragment of alpha-melanocyte-stimulating hormone (alpha-MSH) with potent anti-inflammatory properties. Its role in injury recovery is inflammation control, specifically reducing the excessive or prolonged inflammation that delays healing and causes secondary tissue damage.
The mechanism centres on NF-kB inhibition. NF-kB is the master switch for inflammatory gene expression, and KPV directly suppresses its activation. This reduces pro-inflammatory cytokine production (TNF-alpha, IL-6, IL-1beta) without completely shutting down the inflammatory process that is necessary for initial wound cleaning. The result is modulated inflammation rather than suppressed inflammation, which is a critical distinction for recovery outcomes.
KPV is particularly relevant for injuries with a strong inflammatory component: acute sports injuries with significant swelling, post-surgical inflammation, inflammatory joint conditions, and chronic overuse injuries where persistent low-grade inflammation is preventing tissue repair. It also has documented benefits for gut inflammation, making it a natural complement to BPC-157's gut health applications when gastrointestinal stress accompanies injury recovery (common in athletes on NSAIDs).
Standard dosing is 200-500mcg subcutaneously, once daily. KPV can be run alongside BPC-157 and TB-500 as part of a comprehensive protocol where inflammation management is a priority. It is newer to the recovery peptide conversation than BPC-157 or TB-500, but the research on its anti-inflammatory mechanism is robust and its clinical applications are expanding.
Best for: Acute injuries with significant inflammation, post-surgical swelling, chronic inflammatory conditions delaying recovery, overuse injuries, and as an NSAID alternative for inflammation management during peptide recovery protocols.
How to Choose the Right Recovery Peptide
The right peptide depends on your injury type, severity, and recovery goals. For a single localised injury like a torn tendon or strained muscle, BPC-157 alone is the most targeted and evidence-backed starting point. For more severe injuries or multi-site damage, the Wolverine Stack (BPC-157 + TB-500) is the standard recommendation in peptide therapy clinics.
Where to source it
The hard part with BPC-157 isn't the protocol. It's finding a supplier that can prove what's in the vial. We assessed dozens against per-batch, third-party testing. A handful passed.
See the sources that passed →Adding GHK-Cu makes sense when tissue quality and scar management matter, particularly after surgery or in injuries where collagen integrity is critical (tendons, ligaments, skin). CJC-1295/Ipamorelin adds value for patients over 35-40 whose natural growth hormone levels are declining, or for any recovery where lean mass preservation is a priority.
Thymosin Alpha-1 and KPV are adjuncts rather than primary recovery peptides. Thymosin Alpha-1 fills a gap when immune function is limiting recovery speed. KPV fills a gap when inflammation is the primary barrier to healing.
Recovery Protocol Stacking Guide
| Injury Scenario | Recommended Peptides | Duration |
|---|---|---|
| Simple muscle strain or minor tendon injury | BPC-157 alone | 4-6 weeks |
| Moderate injury (partial tear, significant sprain) | Wolverine Stack (BPC-157 + TB-500) | 6-8 weeks |
| Post-surgical recovery (ACL, rotator cuff) | Wolverine Stack + GHK-Cu | 8-12 weeks |
| Complex recovery in patients over 40 | Wolverine Stack + CJC-1295/Ipamorelin | 8-12 weeks |
| Chronic non-healing injury with inflammation | BPC-157 + KPV + Thymosin Alpha-1 | 8-12 weeks |
Preparation and Administration Basics
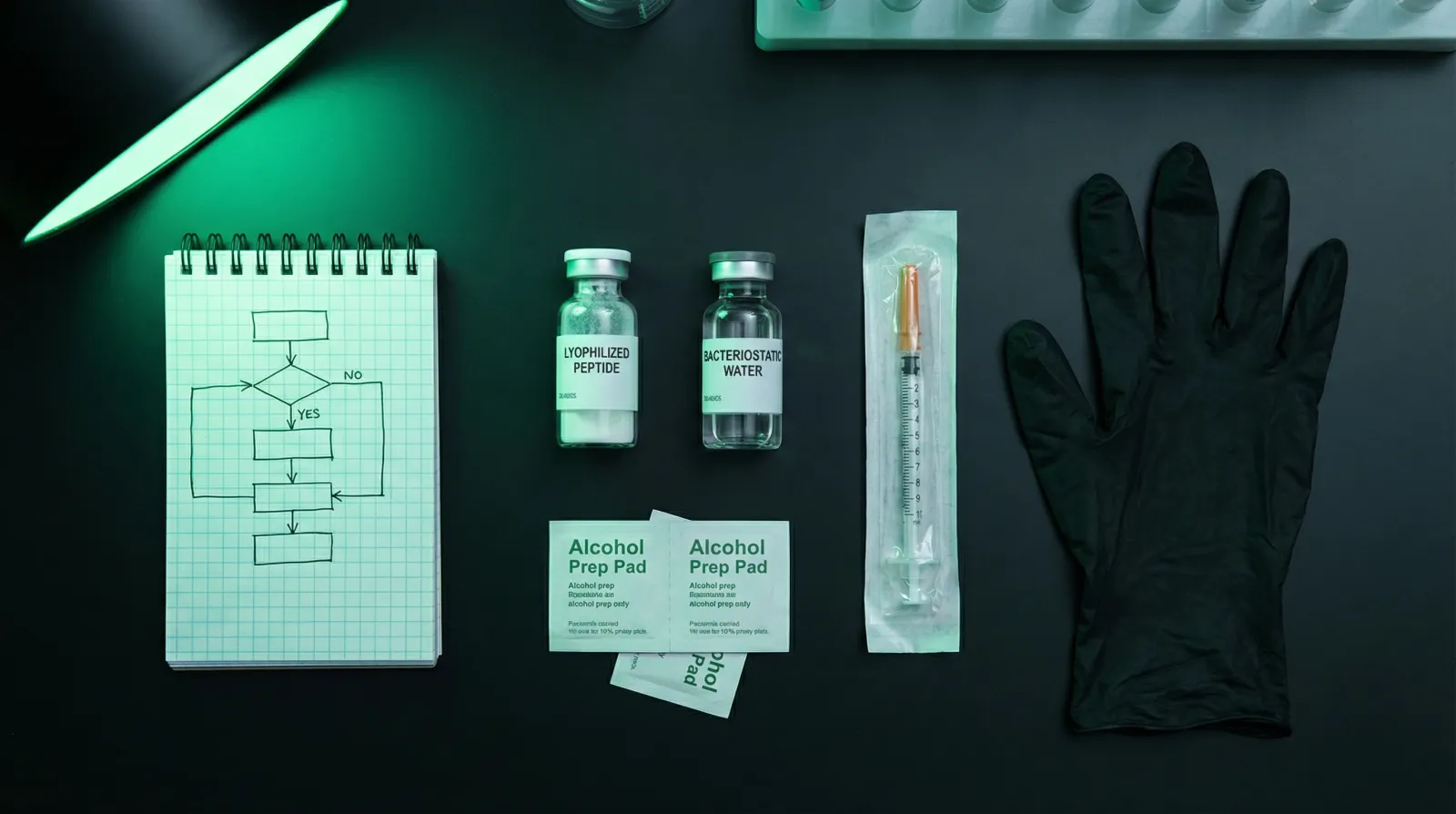
All injectable peptides require reconstitution from lyophilised (freeze-dried) powder using bacteriostatic water before use. If you are new to peptide preparation, our step-by-step reconstitution guide covers the full process including dosage calculations, sterile technique, and storage. This is a non-negotiable prerequisite before starting any peptide protocol.
Sourcing matters enormously for recovery outcomes. With the 2026 FDA reclassification, several of these peptides are now available through licensed compounding pharmacies with purity testing and proper quality control. This is a significant improvement over the research chemical market, and we strongly recommend the compounding pharmacy route for any therapeutic use.
The Bottom Line
Peptide therapy for injury recovery is no longer experimental. BPC-157 and TB-500 have the deepest evidence base and the longest practical track record. GHK-Cu, CJC-1295/Ipamorelin, Thymosin Alpha-1, and KPV each address specific aspects of recovery that the primary healing peptides do not cover. The most effective approach matches the peptide to the injury rather than running everything at once. Start with the compound that targets your specific bottleneck, and add adjuncts only when the recovery context warrants it.
Where to source it
The hard part with BPC-157 isn't the protocol. It's finding a supplier that can prove what's in the vial. We assessed dozens against per-batch, third-party testing. A handful passed.
See the sources that passed →Share this article
Frequently Asked Questions
What is the best peptide for injury recovery?
Can you stack multiple recovery peptides together?
How long does peptide therapy take to work for injuries?
Are recovery peptides legal in 2026?
Do I need to inject peptides near the injury site?
Can I keep training while running a recovery peptide protocol?
Read Next

Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.