
BPC-157 and TB-500 Post-Surgery Recovery Protocol: When to Start, Dosing, and Cycle Length (2026)

BPC-157 and TB-500 Post-Surgery Recovery: What the Stack Actually Does
BPC-157 and TB-500 are the most-evidenced peptide stack for accelerating post-surgical soft-tissue recovery in 2026. Used together for 4 to 8 weeks after orthopaedic, gut, or general surgery, they shorten healing time, reduce inflammation, and support stronger tissue remodelling. They do not replace standard post-op care. They sit alongside it.
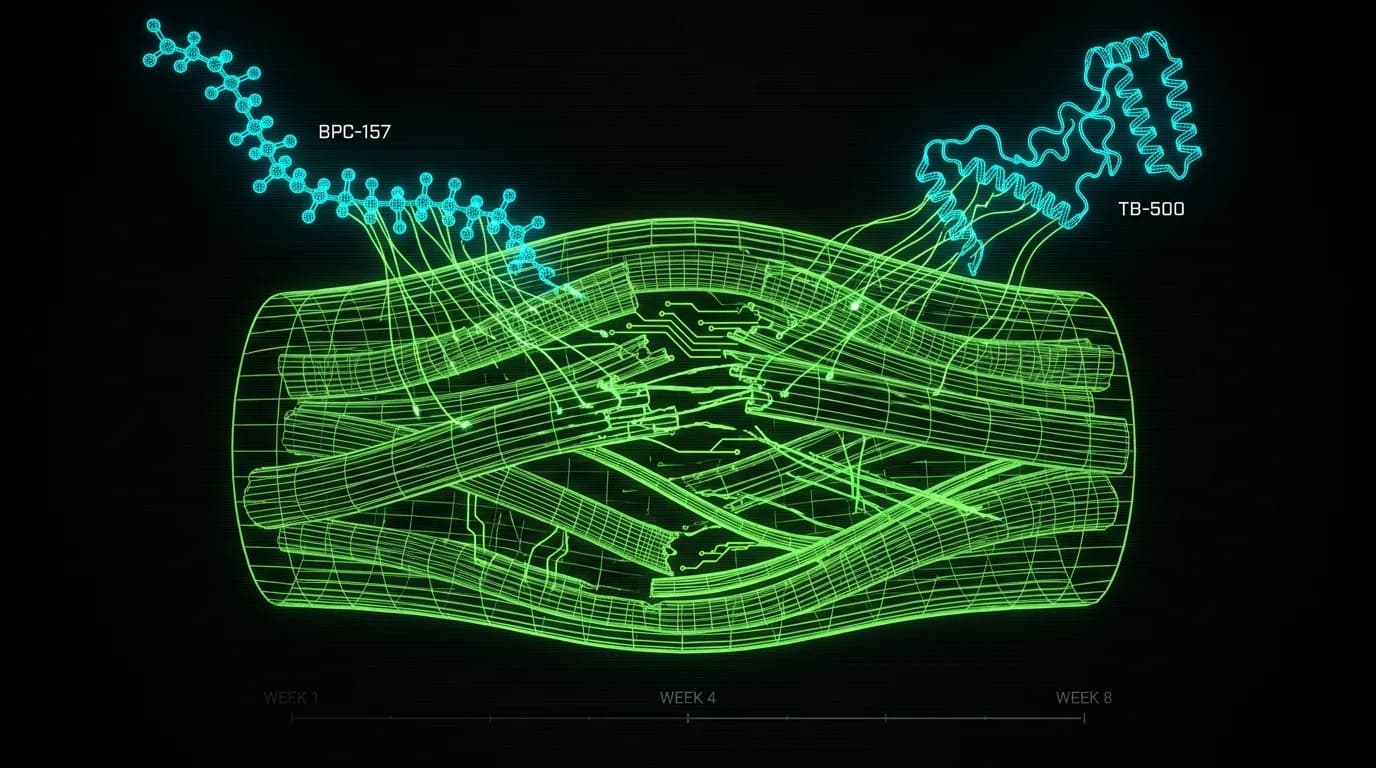
Post-surgical recovery is two parallel processes: damage clearance and tissue rebuild. The first 72 hours are dominated by inflammation and clot formation, the next two weeks by proliferative repair, the following 4 to 8 weeks by remodelling. BPC-157 supports angiogenesis and gut-systemic stability. TB-500 supports cellular migration and actin remodelling. They hit different parts of the same problem.
This is the protocol most recovery clinicians I respect actually run, with the dosing, timing, and cycle length specifics. It also covers the contraindications surgeons care about most.
Why This Stack and Not Just One Peptide
BPC-157 alone is excellent. TB-500 alone is excellent. The case for stacking comes from how their mechanisms layer.
BPC-157, a 15-amino-acid sequence derived from gastric juice, drives angiogenesis, modulates the nitric oxide system, and supports gut-vascular integrity. The angiogenic action is directly relevant to post-surgical wounds because new blood vessels are the rate-limiting step for tissue oxygenation in any deep repair. BPC-157 also has well-documented protective effects on tendon, ligament, and gut tissue, which covers most of what gets disturbed in elective and trauma surgery.
TB-500 is a synthetic fragment of thymosin beta-4, the most abundant intracellular peptide in the human body. Its primary mechanism is upregulating actin-G to actin-F polymerisation, which drives cellular migration into damage zones. Where BPC-157 helps the blood supply reach the tissue, TB-500 helps the cells get to the right places to rebuild it. TB-500 also has anti-inflammatory and anti-fibrotic effects, which matters because excessive scarring is the most common bad outcome from any surgery that involves muscle, tendon, or fascia.
Stacked, the two peptides cover angiogenesis and cellular trafficking with limited mechanistic overlap. That is the usual argument for combination protocols. Recovery clinicians who have run both peptides on hundreds of post-op patients report consistently faster return-to-function timelines than either alone.
When to Start: The 24 to 72 Hour Window
The standard timing is between 24 and 72 hours after surgery, once primary haemostasis is settled. Starting earlier than 24 hours risks interfering with normal clot formation, particularly with TB-500 which has subtle anti-coagulant signals through its effects on the actin cytoskeleton. Starting later than 72 hours misses the early proliferative window where angiogenesis is most actively forming.
Two specific timing exceptions. Gastrointestinal surgery, where some clinicians delay BPC-157 start until at least 48 hours post-op to allow the surgical anastomosis to begin sealing. Major vascular surgery, where the haemostasis question dominates and timing should always be confirmed by the surgical team.
For routine orthopaedic surgery (knee arthroscopy, rotator cuff repair, ACL reconstruction) the 48-hour mark is the typical clinical default. Confirm with the surgical team. Always.
The Loading Phase: First Two Weeks
The loading phase is high-frequency dosing to saturate the recovery window. The standard protocol pairs both peptides at the upper end of their dose ranges, daily for BPC-157 and twice weekly for TB-500.
BPC-157. 500 mcg twice daily, subcutaneous. Inject in the abdomen, rotating sides. Some practitioners inject near the surgical site for orthopaedic recovery, particularly tendon and ligament work, on the theory that local tissue concentration supports the localised repair. Systemic dosing in the abdomen is the more common default and the evidence supports it.
TB-500. 5 mg twice weekly, subcutaneous, in the abdomen. Higher single doses with lower frequency reflect TB-500 longer half-life and slower mechanism. Some protocols front-load with 10 mg in the first dose, but the safety margin is unclear and the loading benefit is modest.
Run this for 14 days. Track recovery markers (pain at rest, range of motion, swelling, surgical-site appearance) daily. Most patients notice meaningfully faster reduction in swelling and pain during the loading phase.
The Maintenance Phase: Weeks 3 to 8
Once the inflammatory phase has passed and proliferative repair is well underway, the dosing tapers. Maintenance keeps the rebuilding machinery active without over-driving angiogenesis or saturating the actin response.
BPC-157. 250 mcg once daily, subcutaneous. Continue in the abdomen.
TB-500. 2.5 mg once weekly, subcutaneous. Some protocols drop TB-500 entirely after week 4 if recovery is on a strong trajectory. The reasoning is that the cellular migration window is largely closed by then, and remaining TB-500 dosing has diminishing returns.
Total cycle length depends on surgery type. Soft-tissue procedures: 4 to 6 weeks total. Orthopaedic: 6 to 8 weeks. Major reconstructions: extend to 12 weeks if the surgical team is supportive and recovery markers are still improving.
Stacking with Other Recovery Tools
The peptides do not work alone, even when they work well. Recovery is a system. The basics still carry most of the load: protein at 1.6 to 2.0 grams per kilogram of bodyweight, sleep at 8 hours minimum, gentle progressive movement as soon as cleared, and absolute compliance with the surgical team loading and immobilisation protocol.
Beyond the basics, three complementary peptides come up frequently in recovery stacks. GHK-Cu for skin and connective tissue gene expression, often added topically for any visible incision sites. Thymosin alpha-1 for immune support during the post-op vulnerability window, particularly in patients over 60. CJC-1295 with ipamorelin for adults whose growth hormone axis is already declining and who need the GH-driven IGF-1 effect on collagen synthesis. The CJC-1295 + ipamorelin guide covers the protocol detail. The GHK-Cu complete guide covers the topical and injectable applications.
Standard supplements that complement the stack: vitamin C at 500 to 1000 mg daily for collagen synthesis cofactor support, magnesium glycinate at bedtime for sleep quality and muscle relaxation, and a clean omega-3 source for resolution-phase inflammation control.
Side Effects and Risk Profile
Both peptides are well tolerated in published preclinical and clinical observation work. The most common reactions are mild injection-site responses (transient redness, slight warmth, occasional pinpoint bruising). These resolve in 48 hours.
BPC-157: rare reports of mild dizziness on the first dose, occasional reports of injection-site discomfort. No significant systemic side effects in the literature.
TB-500: occasional reports of mild lethargy in the first week, particularly at the higher loading doses. The mechanism is unclear but the effect resolves with maintenance dosing.
The hard contraindications matter more than the side effect profile. Active cancer is a no. Recent cancer surgery is a no, because both peptides promote angiogenesis, and angiogenesis is one of the hallmarks of cancer growth. Pregnancy is a no, on insufficient data. Known allergies to peptide formulations or the bacteriostatic water diluent are obvious nos.
WADA banned BPC-157 in 2022 for athletes, and TB-500 has been on the prohibited list since 2009. Anyone subject to drug testing in regulated sport should not use either peptide post-surgery, regardless of the medical case for them.
What Surgery Types This Protocol Suits
This protocol is most evidence-aligned for orthopaedic soft-tissue surgery: rotator cuff repair, ACL or meniscus reconstruction, Achilles repair, hip or shoulder labrum work, and tendon transfers. The mechanistic case is strongest where soft-tissue repair, tendon-bone interface healing, and inflammation control matter most.
Gut surgery is the second-strongest fit. BPC-157 specific gastric-protective and intestinal-anastomotic-supportive effects are well-documented. TB-500 role is smaller in gut work but the anti-inflammatory contribution is still useful. Always defer to the surgical team on timing for any procedure involving anastomosis.
The protocol is less appropriate, though not contraindicated, for purely cosmetic surgery, dental implants, or skin-only procedures. For those, GHK-Cu topical alone is often the more sensible peptide choice. The best peptides for injury recovery guide covers these alternative protocols.
Sourcing and Quality Control
Post-surgical patients have lower margin for vial contamination than recreational users. Source through a 503A compounding pharmacy under prescription wherever possible, particularly with the 2026 FDA reclassification expanding legal pharmacy access for both peptides. Pharmacy-compounded vials come with sterility validation, identity testing, and a prescribing clinician already involved in the recovery plan.
If pharmacy access is not available, a verified research-grade source with independent third-party certificates of analysis is the practical alternative. Verify the lot-specific COA before reconstitution. The peptide reconstitution guide covers the technique.
The Bottom Line
BPC-157 and TB-500 stacked, dosed correctly, started in the 24 to 72 hour post-op window, run for 4 to 8 weeks total, with a clean loading and maintenance taper, supports faster return to function in most soft-tissue and orthopaedic surgical recoveries. They are an assist, not a substitute. The basics still win. The peptides multiply what the basics build.
Work with a clinician who knows what they are doing. Source through a licensed pharmacy. Verify contraindications before the first dose. Then stop reading and start healing.
Where to source it
The hard part with BPC-157 and TB-500 isn't the protocol. It's finding a supplier that can prove what's in the vial. We assessed dozens against per-batch, third-party testing. A handful passed.
See the sources that passed →Bibliography and Sources
- Sikiric P et al. Stable Gastric Pentadecapeptide BPC 157 in Trauma and Sepsis. Inflammopharmacology, 2018.
- Chang CH et al. The promoting effect of pentadecapeptide BPC 157 on tendon healing. Journal of Applied Physiology, 2011.
- Goldstein AL et al. Thymosin beta4: actin-sequestering protein moonlights to repair injured tissues. Trends in Molecular Medicine, 2005.
- Crockford D et al. Thymosin beta4: structure, function, and biological properties supporting current and future clinical applications. Annals of the New York Academy of Sciences, 2010.
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks. FDA, 2024 update.
Compliance Disclaimer
This article is for informational and educational purposes only and is not medical advice. Peptide compounds discussed are intended for research use unless prescribed by a qualified clinician through a licensed compounding pharmacy. They are not approved by the FDA as finished drug products and are not approved for use in healthy adults outside of legitimate medical indications. Use of any peptide post-surgery should be coordinated with your surgical team and the prescribing clinician. Individual response varies. The strength of evidence is preclinical and observational for many of the claims discussed. Verify current FDA classifications and your state pharmacy board rules before making decisions about access or use.
Where to source it
The hard part with BPC-157 and TB-500 isn't the protocol. It's finding a supplier that can prove what's in the vial. We assessed dozens against per-batch, third-party testing. A handful passed.
See the sources that passed →Share this article
Frequently Asked Questions
When can I start BPC-157 and TB-500 after surgery?
Can I use BPC-157 and TB-500 together?
How long should the recovery cycle run?
Are there risks to using these peptides during cancer recovery?
Subcutaneous or intramuscular injection?
Can these peptides replace post-op physical therapy?
Read Next

Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.