
KPV Complete Guide: The Alpha-MSH Fragment, NF-kB Inhibition, and Anti-Inflammatory Mechanism (2026)

What Is KPV Peptide? The Alpha-MSH Fragment Redefining Immune Modulation
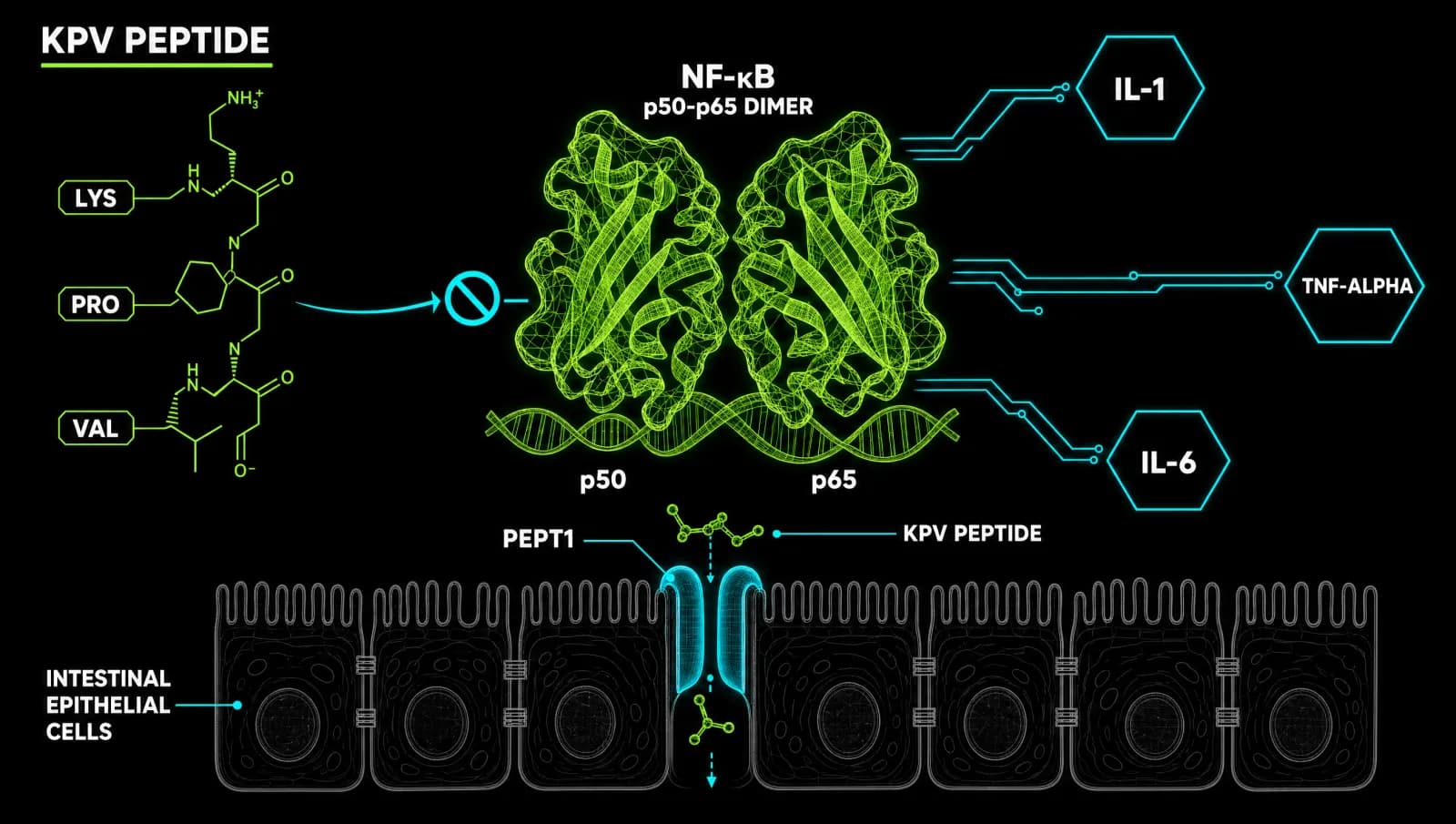
KPV peptide is a three-amino-acid fragment (Lysine-Proline-Valine) cleaved from the C-terminal end of alpha-melanocyte-stimulating hormone (alpha-MSH). It inhibits NF-kB, suppresses pro-inflammatory cytokines, and enters gut epithelial cells via PepT1 transporters, making it one of the most mechanistically precise anti-inflammatory peptides in current research. (Dalmasso 2008)
If you have spent time researching gut inflammation, skin conditions, or immune dysregulation, you have likely encountered KPV referenced alongside BPC-157 or GHK-Cu. But KPV operates through a distinct and well-characterised pathway that sets it apart from every other peptide in this category. It is not a growth factor. It is not a repair signal. It is a direct molecular brake on the NF-kB inflammatory cascade, derived from a neuropeptide your own immune system already uses.
This guide covers the full mechanistic picture: what KPV is, where it comes from, how it silences inflammation at the transcription level, what the preclinical data actually says about gut health and antimicrobial defence, and how it sits alongside other tools in a research-informed protocol.
Affiliate disclosure: This post contains links to third-party research compound suppliers. Underground Biohacking may earn a commission if you purchase through those links, at no additional cost to you. We recommend only suppliers we have vetted for purity documentation. See our recommended sources for our current vendor list.
The Origins of KPV: POMC, Alpha-MSH, and the C-Terminal Fragment
KPV originates from proopiomelanocortin (POMC), a precursor protein cleaved by the body into multiple bioactive peptides, one of which is alpha-MSH. The C-terminal three amino acids of alpha-MSH, positions 11 through 13, are Lysine-Proline-Valine. This fragment retains the core anti-inflammatory and immunomodulatory activity of the parent molecule. (Brzoska 2008)
Alpha-MSH itself is a 13-amino-acid neuropeptide produced in the pituitary gland and peripheral tissues. It binds melanocortin receptors (MC1R through MC5R) distributed across immune cells, skin, gut, and the central nervous system. Researchers identified decades ago that much of alpha-MSH's anti-inflammatory potency resided in the C-terminal region, specifically the tripeptide KPV.
The significance of this discovery is practical. A tripeptide is stable, orally bioavailable under the right conditions, small enough to cross epithelial barriers via peptide transporters, and cheap enough to study at scale. The full 13-amino-acid alpha-MSH degrades rapidly and presents delivery challenges. KPV side-steps most of those problems while preserving the core mechanism.
As Singh and Mukhopadhyay (2014) established in their comprehensive PMC review, alpha-MSH C-terminal fragments including KPV exhibit parallel antimicrobial and immunomodulatory properties to the full peptide. The POMC-melanocortin axis is not a niche pathway. It is a central regulator of immune homeostasis that the body activates under inflammatory stress.
NF-kB Inhibition: The Master Switch KPV Targets
KPV peptide suppresses inflammation by directly inhibiting NF-kB, the transcription factor that controls expression of hundreds of pro-inflammatory genes including those encoding IL-1, IL-6, TNF-alpha, and COX-2. By blocking NF-kB activation, KPV reduces inflammatory output at the source rather than neutralising individual cytokines downstream. (Catania et al. 2000)
NF-kB sits at the convergence point of nearly every major inflammatory signalling cascade. Pattern recognition receptors (toll-like receptors, NOD receptors), cytokine receptors, and oxidative stress signals all feed into NF-kB activation. Once NF-kB translocates to the nucleus, it triggers transcription of inflammatory mediators that amplify the immune response. In chronic conditions, this becomes self-sustaining: cytokines activate NF-kB, NF-kB produces more cytokines.
KPV interrupts this loop. A 2025 study by Sung et al. published in Tissue and Cell demonstrated that KPV directly modulates both MAPK and NF-kB signalling pathways to reduce oxidative stress and keratinocyte apoptosis caused by fine dust particulate matter. The researchers identified dual pathway suppression: KPV blocked phosphorylation events upstream of NF-kB activation while simultaneously reducing reactive oxygen species that would otherwise sustain the inflammatory loop.
Earlier mechanistic work by Lipton et al. 1997 showed alpha-MSH inhibits fever and acute inflammation through both central neural pathways and peripheral immune cell signalling. The mechanism is mediated through melanocortin receptors on macrophages and neutrophils, with KPV acting as an effective ligand for this receptor family. This dual central-peripheral action distinguishes KPV from conventional anti-inflammatories that operate only at the site of tissue damage.
PepT1-Mediated Gut Entry: Why KPV Is Uniquely Suited to Intestinal Inflammation
KPV enters intestinal epithelial cells via PepT1, a peptide transporter that normally shuttles small dietary peptides across the gut lumen. This active transport mechanism means KPV is absorbed intact into gut tissue, where it can suppress local NF-kB activation directly in the inflamed epithelium, rather than requiring systemic circulation to reach its target. (Dalmasso 2008)
The Dalmasso 2008 study in Gastroenterology is the landmark paper establishing this mechanism. The researchers demonstrated that KPV uptake via PepT1 reduces intestinal inflammation in cell culture and murine models of colitis. Crucially, they showed that PepT1 expression is upregulated during inflammation, meaning the transporter becomes more available precisely when it is most needed. This is an elegant piece of biological design: KPV's access to inflamed gut tissue improves as inflammation intensifies.
For researchers and clinicians studying inflammatory bowel conditions, this transport mechanism has significant implications. Oral KPV delivery could theoretically achieve local gut concentrations sufficient to suppress NF-kB in inflamed tissue without requiring injectable administration. A 2023 review by Gravina et al. in Cells confirmed that the melanocortin system, including KPV, shows therapeutic potential for inflammatory bowel disease through multiple pathways including epithelial barrier integrity, immune cell modulation, and cytokine suppression.
Cytokine Suppression Profile: IL-1, IL-6, TNF-Alpha
KPV suppresses three of the most clinically relevant pro-inflammatory cytokines: interleukin-1 (IL-1), interleukin-6 (IL-6), and tumour necrosis factor-alpha (TNF-alpha). These are the same targets addressed by biologic drugs costing tens of thousands of pounds annually. KPV achieves this suppression through upstream NF-kB inhibition rather than receptor blockade. (Macaluso et al. 1994, Lipton et al. 1997)
The 1993 study by Catania et al. established that KPV (alpha-MSH 11-13) inhibits inflammation when administered systemically, acting through both central neurogenic mechanisms and peripheral tissue sites. This work predates many of the biologic drug approvals that now dominate rheumatology and gastroenterology. It positions KPV as a naturally derived molecule that targets the same inflammatory nodes as pharmaceutical biologics, through a different mechanism.
The distinction matters clinically. TNF-alpha inhibitors (adalimumab, etanercept) block the cytokine after it is produced. They do not address the upstream transcription driving its production. KPV's NF-kB inhibition targets production itself. The theoretical advantage is a broader suppression of the inflammatory transcriptome without the immunosuppression associated with blocking a single effector cytokine.
Concentrations of alpha-MSH are increased at sites of inflammation in humans, suggesting the body already deploys this system as a negative feedback regulator of immune activation. KPV can be understood as augmenting an endogenous brake that the body attempts to engage under inflammatory stress. (Lipton et al. 1997)
Antimicrobial Properties: Staphylococcus aureus and Candida Albicans
KPV demonstrates direct antimicrobial activity against gram-positive bacteria including Staphylococcus aureus and the fungal pathogen Candida albicans at physiological, picomolar-to-nanomolar concentrations. Critically, this antimicrobial activity occurs without reducing neutrophil killing capacity, meaning KPV suppresses dysregulated inflammation while preserving functional immune defence. (Cutuli 2000)
This dual profile is unusual. Most anti-inflammatory interventions carry some risk of infection as a trade-off: suppressing immune activity broadly increases susceptibility to pathogens. KPV appears to avoid this trade-off through its specific mechanism. The 2000 study by Cutuli et al. established that KPV's antimicrobial effects are mediated through cAMP elevation in immune cells, which enhances pathogen killing without compromising the neutrophil oxidative burst.
The 2001 work by Bhardwaj et al. further showed that alpha-MSH inhibits NF-kB activation to reduce viral replication in HIV models, with KPV identified as the active fragment. This suggests the peptide's immune modulating effects extend to viral contexts, though this research remains preclinical and is far from clinical translation.
For gut health applications specifically, the antimicrobial dimension is relevant. Inflammatory bowel conditions are often accompanied by dysbiosis and overgrowth of opportunistic pathogens. A compound that simultaneously suppresses mucosal inflammation and maintains antimicrobial defence against S. aureus and C. albicans addresses two problems that typically require separate interventions.
KPV Versus Conventional Anti-Inflammatories: A Mechanism Comparison
KPV operates through melanocortin receptor signalling and cAMP elevation, a fundamentally different mechanism from NSAIDs (COX inhibition), corticosteroids (glucocorticoid receptor activation), or biologic drugs (cytokine or receptor blockade). This mechanistic distinctness means KPV does not share the gastrointestinal, cardiovascular, or broad immunosuppressive side-effect profiles of conventional anti-inflammatory drugs. (Brzoska 2008)
NSAIDs inhibit cyclooxygenase enzymes to reduce prostaglandin synthesis. They are effective for acute inflammation but cause gastrointestinal mucosal damage, increase cardiovascular risk with long-term use, and do nothing for the cytokine cascades driving chronic inflammatory diseases. KPV does not touch COX enzymes.
Corticosteroids bind glucocorticoid receptors ubiquitously and suppress immune function broadly. They are powerful but indiscriminate. Long-term corticosteroid use causes adrenal suppression, bone density loss, insulin resistance, and impairs healing. KPV's melanocortin receptor mechanism is more targeted, acting through specific receptor subtypes on immune cells rather than through the global glucocorticoid programme.
Biologic drugs like TNF-alpha inhibitors are highly specific but expensive, injectable, and carry risks of serious infection due to systemic cytokine suppression. KPV's upstream NF-kB inhibition potentially addresses a broader range of inflammatory mediators through a single mechanism, without blocking effector cytokines that serve protective functions in infection control.
This comparison is not a claim that KPV is superior to approved medications for any specific condition. It is a mechanistic map of where KPV sits in the pharmacological landscape and why it warrants continued research attention. Always work with a qualified clinician before making changes to your health protocol.
Skin and Dermatological Applications: The MAPK-NF-kB Axis
KPV reduces inflammation in skin keratinocytes by modulating both the MAPK signalling pathway and NF-kB activation, reducing oxidative stress and preventing cell apoptosis in response to environmental inflammatory triggers. This dual pathway modulation makes KPV relevant to dermatological research beyond its gut applications. (Sung 2025)
The 2025 Sung et al. study is the most recent and mechanistically detailed investigation of KPV in skin tissue. Using fine particulate matter as the inflammatory stressor, the researchers demonstrated that KPV treatment reduced markers of oxidative stress (ROS, lipid peroxidation), suppressed MAPK phosphorylation (ERK, JNK, p38), and blocked NF-kB nuclear translocation. Cell survival increased and inflammatory cytokine production decreased across all measured endpoints.
Earlier work establishing alpha-MSH's role in skin defence, reviewed by Hiltz et al. 1990, identified antipyretic and anti-inflammatory effects in acute oedema models and contact sensitivity responses. Skin is a melanocortin-rich tissue: keratinocytes, melanocytes, Langerhans cells, and dermal immune cells all express melanocortin receptors. KPV's access to these cells makes the dermatological research particularly plausible mechanistically.
Evidence Quality and Research Status
KPV has strong and consistent preclinical evidence across three decades of PubMed-indexed research, from initial mechanism studies in the 1990s through recent MAPK-NF-kB pathway investigations in 2025. The evidence base is mechanistically coherent across multiple tissue types. Human clinical trials remain limited, which is the primary caveat for any translational claim. (Brzoska 2008)
The research timeline tells a consistent story. From the early 1990s demonstration of systemic anti-inflammatory effects (Macaluso et al. 1994), through the identification of antimicrobial properties at physiological concentrations (Cutuli 2000), through the discovery of PepT1-mediated intestinal uptake (Dalmasso 2008), to the 2025 mechanistic confirmation of dual MAPK and NF-kB modulation (Sung 2025), the evidence is additive rather than contradictory.
Multiple independent research groups across different countries and decades have converged on the same core finding: KPV inhibits NF-kB, suppresses pro-inflammatory cytokines, retains antimicrobial activity, and does so through melanocortin receptor signalling. This convergence is a reasonable indicator of mechanistic validity, even in the absence of large-scale human trial data.
The evidence grade for specific claims:
- NF-kB inhibition: established in multiple preclinical models and mechanistic studies
- PepT1-mediated gut uptake: demonstrated in cell culture and murine colitis models
- Cytokine suppression (IL-1, IL-6, TNF-alpha): preclinical and mechanistic
- Antimicrobial activity: preclinical, picomolar concentrations in vitro
- Human IBD treatment: no completed randomised controlled trials; theoretical basis from preclinical data and melanocortin system reviews
Researchers and clinicians approaching KPV should treat it as a compound with a compelling mechanistic rationale and strong preclinical support, not as an approved therapeutic with established clinical dosing protocols.
KPV in Context: How It Fits Alongside Other Peptides
KPV occupies a specific niche within the peptide research landscape: it is the primary NF-kB targeting option among commonly researched peptides, which positions it as a complement to BPC-157 (which works primarily through growth factor and angiogenesis pathways) and GHK-Cu (which acts through copper-dependent gene regulation). These mechanisms do not overlap significantly, making combination research protocols theoretically synergistic. (Brzoska 2008)
Where to source it
Research-grade KPV from a verified supplier with third-party purity documentation. See our recommended sources before purchasing.
See the sources that passed →BPC-157's primary documented mechanisms involve VEGF signalling, nitric oxide pathways, and growth factor receptor upregulation for tissue repair. GHK-Cu, which we have covered in detail on the blog, operates through copper chaperone activity and broad gene expression modulation affecting over 4,000 genes. KPV's focused NF-kB inhibition is mechanistically distinct from both.
For gut health specifically, the combination of PepT1-mediated KPV entry with BPC-157's mucosal repair effects represents a theoretically rational research approach: address the inflammatory driver (KPV, NF-kB inhibition) alongside the structural repair mechanism (BPC-157, growth factor signalling). This is hypothesis, not clinical guidance. No human trials have examined this combination.
For recommended suppliers of research-grade KPV, see our recommended sources page, which lists vendors with current third-party purity testing documentation.
Frequently Asked Questions
References
- Dalmasso G et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008. PMID 18061177
- Brzoska T et al. Alpha-melanocyte-stimulating hormone and related tripeptides: biochemistry, antiinflammatory and protective effects in vitro and in vivo. Endocrine Reviews. 2008. PMID 18612139
- Bhardwaj RS et al. The Neuropeptide alpha-MSH in Host Defense. 2001. PMID 11268348
- Catania A et al. Antiinflammatory influences of alpha-MSH molecules: central neurogenic and peripheral actions. 1993. PMID 8158274
- Cutuli M et al. Antimicrobial effects of alpha-MSH peptides. 2000. PMID 10670585
- Bhardwaj RS et al. Anti-inflammatory actions of the neuroimmunomodulator alpha-MSH. 1994. PMID 9078687
- Singh M, Mukhopadhyay K. Alpha-Melanocyte Stimulating Hormone: An Emerging Anti-Inflammatory Antimicrobial Peptide. PMC 2014. PMC4130143
- Luger TA et al. Alpha-MSH peptides inhibit acute inflammation and contact sensitivity. 1990. PMID 2284205
- Gravina AG et al. The Melanocortin System in Inflammatory Bowel Diseases. Cells. 2023. PMC10378568
- Sung Y et al. Lysine-Proline-Valine peptide mitigates fine dust-induced keratinocyte apoptosis and inflammation by regulating oxidative stress and modulating the MAPK/NF-kB pathway. Tissue & Cell. 2025. PMID 40073467
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.
Where to source it
Research-grade KPV from a verified supplier with third-party purity documentation. See our recommended sources before purchasing.
See the sources that passed →Share this article
Frequently Asked Questions
What is KPV peptide and how does it work?
How does KPV enter gut cells and exert its anti-inflammatory effects?
What conditions has KPV been researched for?
Does KPV have antimicrobial properties alongside its anti-inflammatory effects?
What is the relationship between KPV and alpha-MSH?
How does KPV compare mechanistically to NSAIDs and corticosteroids?
Read Next


Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.