
KPV for Gut Health: IBD, Gut Inflammation, Oral vs Injectable Protocols (2026)


What Is KPV and Why Gut-Focused Peptide Users Are Watching It
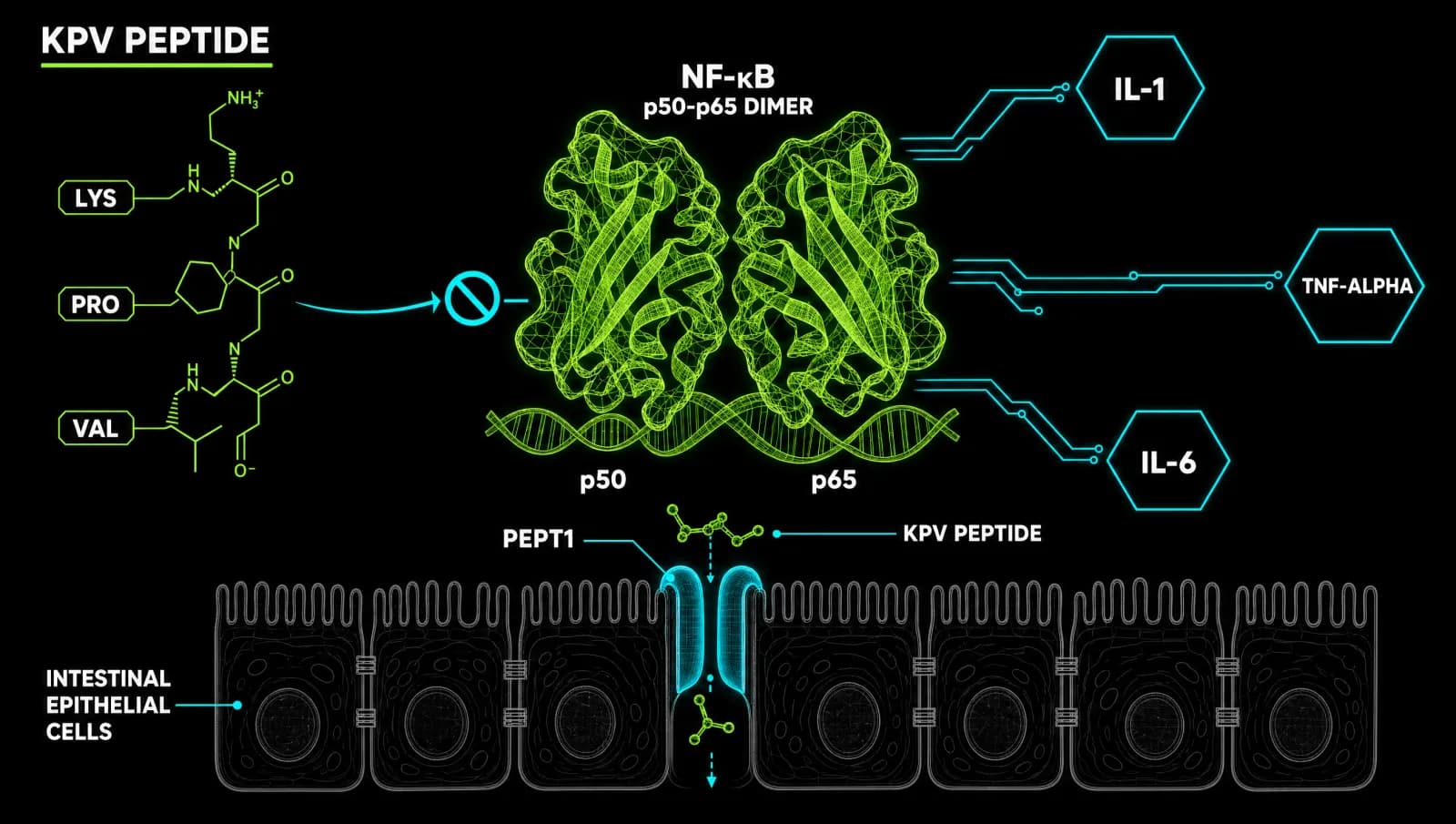
KPV is a tripeptide (Lys-Pro-Val) clipped from the tail end of alpha-melanocyte-stimulating hormone. Research users are watching it because it calms gut inflammation at the cellular level without the broad immune suppression that comes with corticosteroids or NSAIDs, making it a candidate for IBD and general gut-barrier support.
KPV is three amino acids long: lysine, proline, valine. That's the entire molecule. It is the C-terminal fragment of alpha-MSH, and researchers found decades ago that this tiny fragment keeps almost all of the parent hormone's anti-inflammatory punch while dropping the pigmentation and broader hormonal effects that come with the full peptide. Studies confirm KPV retains anti-inflammatory capacity without binding melanocortin receptors and without the skin-darkening side effect seen with full alpha-MSH exposure (Brzoska 2010).
This is a link to a trusted source for KPV research below; it supports the channel and costs you nothing extra.
How KPV Actually Reduces Gut Inflammation
KPV works by blocking NF-kB and MAP kinase, the signalling pathways that switch on inflammation inside gut cells. It gets pulled directly into intestinal tissue through a transporter called PepT1, which the gut upregulates exactly where inflammation is worst, so KPV concentrates in the tissue that needs it most.
Nanomolar concentrations of KPV inhibit NF-kB and MAP kinase activation and cut secretion of pro-inflammatory cytokines including TNF-alpha, IL-1beta and IL-6 (Dalmasso 2008). The transporter mechanism matters more than it looks. PepT1 normally sits in the small intestine, but during active inflammatory bowel disease it gets pushed higher in the colon, the exact tissue under attack. That means inflamed gut lining pulls in more KPV than healthy tissue does, a form of self-targeting that oral dosing takes direct advantage of (Dalmasso 2008).
KPV also modulates neutrophil accumulation independent of melanocortin receptor binding, which is why it behaves differently from its parent hormone in inflammation models (Getting 2003). A dimer form, (CKPV)2, shuts down TNF-alpha production in human immune cells and in vivo endotoxin exposure, reinforcing that this is a genuine cytokine-suppression mechanism rather than a marginal effect (Gatti 2006). Separately, KPV shows antimicrobial activity against Staphylococcus aureus and Candida albicans at physiological picomolar concentrations, which may contribute to gut barrier protection alongside the anti-inflammatory action (Cutuli 2000).
Oral vs Injectable KPV: Which Route Fits Gut Health
For gut-specific inflammation, oral KPV is generally the smarter route because the PepT1 transporter delivers it straight into inflamed intestinal tissue, exactly where you want it. Subcutaneous injection raises systemic exposure and suits broader, non-gut inflammatory targets rather than IBD-specific work.
Oral administration reduces incidence and severity of DSS- and TNBS-induced colitis in animal models, with pro-inflammatory cytokine expression dropping alongside improved tissue architecture (Dalmasso 2008). Oral dosing has lower total systemic bioavailability than an injection, but that is not the point of taking it orally for gut work. The PepT1 route means KPV never has to travel through the bloodstream to reach the colon, it is absorbed directly at the point of inflammation.
Subcutaneous KPV bypasses the gut wall entirely and enters circulation. That is useful if the goal is systemic anti-inflammatory support rather than a gut-specific target, but for IBD or general gut-barrier work the oral route puts the compound where the PepT1 transporter is already primed to pull it in. Plasma half-life after subcutaneous dosing runs around two hours, which is short enough that most protocols split doses across the day rather than relying on a single injection.
KPV Dosing Protocols and Stacking for Gut Healing
Typical oral protocols for gut inflammation run 200 to 500 micrograms up to 1 milligram daily on an empty stomach, with some users pushing toward 1,000 micrograms during an active flare. Subcutaneous protocols for systemic effects sit lower, around 250 to 500 micrograms once or twice daily.
Cycles in the peptide research community typically run 4 to 8 weeks, followed by a break to reassess symptoms rather than continuous year-round use. Anecdotally, users report combining KPV with BPC-157: KPV to bring down the inflammatory signalling and BPC-157 to work on structural repair of the gut lining, since the two are doing different jobs at the same site. Some stacks also add GHK-Cu when skin or connective tissue repair is a secondary goal.
None of this replaces individualised medical guidance. If you are considering a protocol involving dosing changes for a diagnosed gut condition, always work with a qualified clinician before making changes to your health protocol. IBD in particular is a condition where self-directed experimentation without oversight carries real risk.
Safety, Legal Status, and Where This Research Stands in 2026
Preclinical data on KPV point to a favourable safety profile with none of the broad immune suppression seen with corticosteroids, but human trial data remain thin. Regulatory status is also shifting: the FDA's Pharmacy Compounding Advisory Committee reviewed KPV for compounding approval in mid-2026.
The strongest human evidence so far is a pilot trial of intrarectal (topical) KPV in patients with mild to moderate ulcerative colitis, which reported clinically meaningful improvement in disease activity scores. That is a pilot study, not a large randomised controlled trial, and no completed RCT exists yet for KPV in IBD. Nearly everything else in the evidence base sits at the cell-culture or animal-model level, which is a meaningful gap between what the mechanism promises and what has actually been shown in people.
On the regulatory side, KPV's status has been moving. The FDA's Pharmacy Compounding Advisory Committee reviewed it for compounding approval, a step that would let licensed compounding pharmacies legally produce it if approved. That is a different regulatory lane from an FDA-approved drug claim, and nothing here should be read as one.
Sourcing KPV for Research Purposes
If you are researching KPV, source quality determines whether you are actually studying the compound described in these papers or a mislabelled substitute. Third-party testing, clear certificates of analysis, and vendor transparency separate a legitimate research source from the rest of the market.
We keep a vendor-neutral breakdown of what to check before buying any research peptide on our recommended sources page, including how to read a certificate of analysis and what red flags to watch for. If you want a deeper walk-through of verifying peptide authenticity before you ever place an order, see our guide on how to know if peptides are real.
Where to source it
If you're researching this compound, I've linked a trusted source below. It supports the channel.
See the sources that passed →References
- Dalmasso G, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. 2008. PubMed
- Dalmasso G, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation (full text). 2008. PMC
- Getting SJ, Schioth HB, Perretti M. Dissection of the anti-inflammatory effect of the core and C-terminal (KPV) alpha-MSH peptides. 2003. PubMed
- Gatti S, et al. Inhibitory effects of the peptide (CKPV)2 on endotoxin-induced host reactions. 2006. PubMed
- Brzoska T, et al. Terminal signal: anti-inflammatory effects of alpha-MSH related peptides beyond the pharmacophore. 2010. PubMed
- Cutuli M, et al. Antimicrobial effects of alpha-MSH peptides. 2000. PubMed
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.
Where to source it
If you're researching this compound, I've linked a trusted source below. It supports the channel.
See the sources that passed →Share this article
Frequently Asked Questions
What is KPV and where does it come from?
How does KPV reduce gut inflammation?
Is KPV better taken orally or by injection for gut health?
What is the typical KPV dosage for gut inflammation?
Has KPV been tested in humans with IBD?
Is KPV legal to source in 2026?
Read Next

Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.