
How to Inject Peptides: Subcutaneous Technique, Sites, and Safety (2026)

How to Inject Peptides Subcutaneously: The Complete Technique Guide
Subcutaneous peptide injection means placing the needle into the fatty tissue directly beneath your skin, between the dermis and muscle. With the right syringe, correct angle, and basic sterile technique, this is a straightforward skill any man can learn at home in under ten minutes. This guide covers everything from insulin syringe maths to site rotation to safe sharps disposal.
This is a universal guide covering subcutaneous technique across all research peptides. For compound-specific protocols including intramuscular options, see the compound-specific injection techniques guide. For dose calculations before you draw your first syringe, use the dosing calculator.
Affiliate disclosure: This post contains links to recommended suppliers. Underground Biohacking earns a commission on qualifying purchases at no cost to you. We only recommend sources we have personally vetted. See our recommended sources page for the current approved list.
What You Need Before You Start
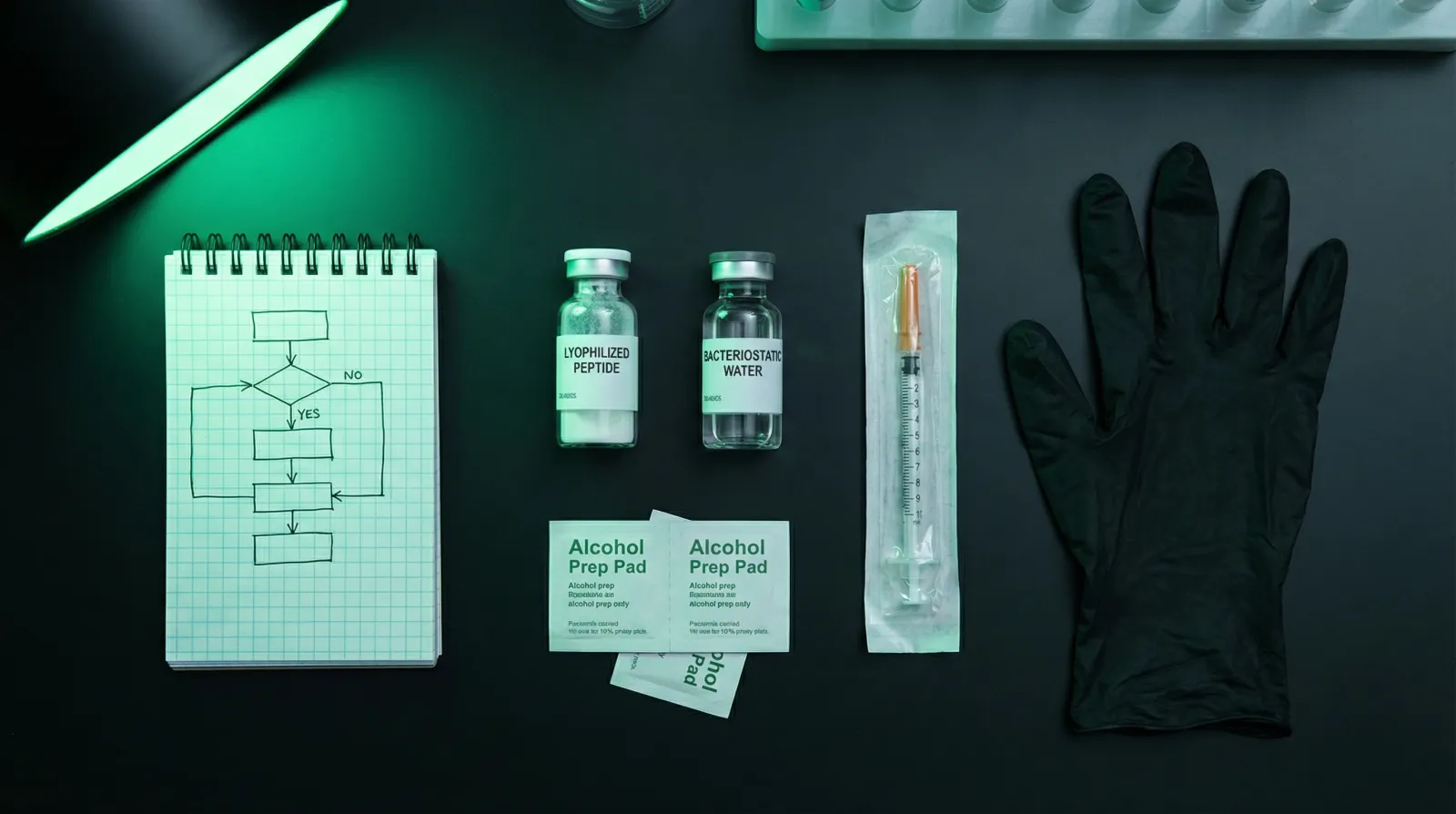
A successful subcutaneous injection requires five items: a U-100 insulin syringe (29–31 gauge, 4–8 mm needle), your reconstituted peptide vial, an alcohol prep pad, a sharps disposal container, and a clean flat surface. Sourcing the wrong needle gauge or omitting the sharps container are the two most common beginner oversights.
Choosing the Right Insulin Syringe
Insulin syringes come in three barrel sizes: 0.3 mL (30 units), 0.5 mL (50 units), and 1.0 mL (100 units). For most peptide research doses in the 100–500 mcg range, the 0.5 mL or 1.0 mL syringe gives you enough precision to read the graduation marks clearly. Needle length should be 4–6 mm for abdominal injections at 90 degrees; 8 mm needles require a pinch technique at 45 degrees (PIC Solution 2024).
Gauge matters for pain. A 29–31 gauge needle is thin enough that most people barely feel insertion. Never use a 25 gauge or thicker syringe for subcutaneous peptide work; the tissue trauma is unnecessary.
One important nuance: standard insulin syringes retain approximately 0.5–1 unit (0.005–0.01 mL) of liquid in the hub after injection. For doses under 5 units, this dead volume represents a meaningful percentage of your total draw. Low dead-volume (LDV) syringes eliminate this and are worth the marginal extra cost if you are working with micro-doses (Peptide Protocol Wiki 2026).
Understanding Insulin Syringe Units vs. International Units (IU)
Syringe units and International Units are completely different systems that beginners routinely confuse. On a standard U-100 insulin syringe, 100 units equals 1 mL, and each unit mark represents 0.01 mL of volume. International Units (IU) measure biological activity, not volume, and the conversion factor is completely peptide-specific.
On a U-100 insulin syringe, 100 units = 1 mL; each unit mark = 0.01 mL. This is a volume measurement, full stop (Peptide Reference 2026).
International Units measure bioactivity, and the relationship between mass and IU is different for every compound: HGH converts at 1 mg = 3 IU; HCG converts at roughly 1 mg = 10,000 IU; human insulin converts at 1 mg = 26.11 IU (Real Peptides 2026). These conversion factors cannot be extrapolated from one peptide to another.
The practical error this causes: a researcher with a 500 IU HCG dose assumes they draw to the 500 line on the syringe. They do not. They calculate the volume containing 500 IU based on the vial's concentration, then draw that volume in syringe units (Peptide Protocol Wiki 2026). Most research peptides (BPC-157, TB-500, ipamorelin, CJC-1295) are dosed in micrograms or milligrams rather than IU, which sidesteps this confusion entirely (Real Peptides 2026).
The Three-Step Dose Calculation
Use this formula every time you draw a new peptide or change reconstitution volume:
- Concentration: Peptide amount (mcg) ÷ Water added (mL) = mcg/mL
- Volume needed: Desired dose (mcg) ÷ Concentration (mcg/mL) = mL
- Syringe units: Volume (mL) × 100 = units to draw
Example: 5 mg (5,000 mcg) peptide reconstituted with 2.5 mL bacteriostatic water = 2,000 mcg/mL concentration. A 200 mcg dose requires 0.1 mL, which is 10 units on the syringe (Dosage Tools 2026).
For the full reconstitution walkthrough before you reach this step, see the peptide reconstitution guide.
Reconstitution Recap: Aseptic Technique in Five Steps
Peptide reconstitution requires bacteriostatic water, two alcohol prep pads, and strict aseptic handling. Research published by the American Peptide Society found that peptides reconstituted with non-sterile diluents showed bacterial contamination within 72 hours. Bacteriostatic water (BAC water), which contains 0.9% benzyl alcohol, prevents this and keeps a multi-dose vial stable for approximately 28 days at 2-8°C refrigeration.
- Wash hands thoroughly. Lay out supplies on a clean surface.
- Swab both rubber stoppers with alcohol prep pads. Allow 30 seconds to air dry completely.
- Draw the calculated volume of bacteriostatic water into your syringe.
- Insert the needle into the peptide vial and inject the water slowly down the inside wall of the vial. Never aim the stream directly at the lyophilised powder and never shake the vial (Next Health 2024).
- Gently swirl (do not shake) until the powder dissolves to a clear solution. Label the vial with the reconstitution date. A properly reconstituted peptide should be clear and free of visible particles; cloudiness or discoloration means do not inject (Extension Health 2026).
BAC water peptides are stable approximately four weeks refrigerated at 2-8°C for most compounds (Seek Peptides 2026). Oxidation-sensitive peptides (those containing cysteine, methionine, or tryptophan residues) may degrade faster; check the compound's stability data. Store vials upright, sealed, and away from light. Do not freeze a reconstituted peptide.
Injection Site Selection and Rotation
The abdomen and outer upper thighs are the two primary sites for self-administered subcutaneous peptide injections. Both offer adequate fatty tissue, good visibility, and easy access without assistance. Repeated injections at the same spot cause scarring and hardening of fatty tissue that interferes with absorption, so systematic site rotation is not optional.
The Abdomen
The abdominal zone runs from two inches out from your navel in all directions, below your ribs, and down to the top of the iliac crest. Stay at least two inches from the navel; the tissue around the umbilicus is denser and more sensitive (Brello Health 2026).
Clinical data shows abdominal injections produce less leakage than thigh injections and that 90-degree needle insertion in the abdomen causes less leakage than 45-degree insertion in the same site (Gradel 2016). For most men with a normal BMI, 90 degrees at the abdomen with a 4–6 mm needle is the default technique.
The Thighs
Use the front-outer third of the upper thigh, roughly the middle third of the thigh's length. Sit down to relax the quadriceps before injecting; a contracted muscle makes tissue harder to pinch and increases discomfort (Peptides Wiki 2026). Avoid the inner thigh, which has a higher concentration of vessels and nerve endings.
The Upper Arms (Caregiver or Training Site)
The posterior lateral upper arm (three inches below the shoulder, above the elbow) is an approved subcutaneous site but is difficult to self-administer accurately (Wisconsin Technical College System 2023). Reserve this site for supervised training or when a partner is available.
Rotation Protocol
Repeated injections at the same spot cause scarring and hardening of fatty tissue that will interfere with absorption (FDA Trial Protocol NCT02621931 2024). The minimum spacing between adjacent injections is one inch; two centimetres is safer. A practical system: divide your abdomen into a mental grid of four to six zones and rotate through them clockwise. When all abdominal zones have been used once, switch to thighs for a session before returning.
Avoid any site that is bruised, reddened, swollen, scarred, or shows stretch marks (Fella Health 2026). Injecting into compromised tissue reduces absorption and increases complication risk.
Step-by-Step Injection Technique
The injection itself takes under 60 seconds when your preparation is solid. The sequence is: wash hands, draw the dose, clean the site, pinch the skin, insert the needle bevel-up at the correct angle, inject slowly, wait three to six seconds, withdraw, apply gentle pressure. That sequence, repeated consistently, is the entire skill.
Step 1: Wash and Prepare
Wash hands for at least 20 seconds with soap and water. Lay out your labelled vial, a fresh insulin syringe still in packaging, one alcohol prep pad, a cotton ball or gauze, and your sharps container within reach.
Step 2: Draw the Dose
Swab the peptide vial rubber stopper with an alcohol prep pad. Allow 30 seconds to dry. Insert the needle through the stopper, invert the vial, and draw slightly past your target unit mark. Remove any air bubbles by tapping the barrel and pushing the plunger to the exact unit mark. Keep the needle sheathed until you are ready to inject.
Step 3: Prepare the Injection Site
Outside a clinical setting, rubbing alcohol on the skin before self-injection is optional rather than mandatory; the infection risk of subcutaneous injection is extremely low when hands and skin are clean (WikiProjectMed 2024). If you prefer alcohol, use a prep pad and allow 30 seconds to air dry before injecting. Wet alcohol on the skin stings.
Step 4: Pinch the Skin Fold
With your non-dominant hand, grasp the skin at your chosen site and lift a skin fold. If you can pinch approximately two inches (50 mm) of tissue, use 90-degree insertion. If you can only pinch about one inch (25 mm), use 45-degree insertion (Drugs.com 2024). A pinch fold is important regardless of needle angle; it creates a defined fatty layer and reduces the chance of inadvertent intramuscular injection.
Step 5: Insert the Needle
Hold the syringe like a pencil or dart. Orient the needle with the bevel (the angled cut) facing upward; inserting point-first rather than bevel-down reduces pain noticeably (Great Ormond Street Hospital 2024). Insert with one smooth, confident motion at your chosen angle (45 or 90 degrees). Full needle insertion is standard: the tip must be deeper than the dermis but not into the underlying muscle (FDA Trial Protocol NCT05275010 2024).
Step 6: Inject Slowly and Wait
Release the pinch fold once the needle is inserted. Press the plunger slowly and steadily. Do not rush; a slow injection distributes the fluid more evenly through the fatty tissue and reduces local irritation. After the plunger reaches the bottom, wait three to six seconds before withdrawing. This brief wait significantly reduces leakage from the injection site (Gradel 2016).
Step 7: Withdraw and Apply Pressure
Withdraw the needle at the same angle it was inserted. Apply gentle pressure with a cotton ball or gauze for a few seconds. Do not rub vigorously; rubbing can cause bruising and disperse the peptide from the intended tissue depot.
Common Beginner Mistakes and How to Avoid Them
The most consequential beginner mistakes are not technique errors: they are maths errors and sterility errors. Confusing syringe volume units with International Units leads to significant under-dosing or over-dosing. Reusing needles introduces bacteria and dulls the tip, causing unnecessary tissue damage and raising infection risk with each subsequent use.
Mistake 1: Confusing Units and IU
The syringe unit-versus-IU confusion is the single most common maths error in peptide research. Syringe units are always a volume measurement (100 units = 1 mL). IU is a bioactivity measurement that is compound-specific and cannot be generalised. If your protocol is in micrograms or milligrams, you never need to think about IU at all. If it is in IU, calculate the volume first using the peptide-specific conversion factor, then convert to syringe units (Peptide Reference 2026).
Mistake 2: Reusing Needles
Every injection requires a fresh, sterile needle. Reusing a needle introduces bacteria, dulls the tip (a single-use needle has a micro-polished point that blunts after one puncture), and raises infection risk significantly (Vaccine Allergy 2025). The cost of a 100-pack of insulin syringes is negligible. There is no justification for reuse.
Mistake 3: Ignoring Purity in Reconstitution Calculations
A vial labelled 10 mg does not necessarily contain 10 mg of active peptide. A vial at 98.2% purity contains 9.82 mg of active peptide; the remainder is moisture, residual salts, and truncated sequences. Calculate active mass before reconstitution to avoid systematically under-dosing every injection across an entire protocol (Real Peptides 2026).
Mistake 4: Injecting Cloudy or Discoloured Solution
A properly reconstituted peptide is clear and colourless, free of visible particles. Cloudiness, yellow or brown discolouration, or floating particles indicate degradation. Do not inject it. Discard the vial (Extension Health 2026).
Mistake 5: Skipping Site Rotation
Injection-site reactions are minimised when injections are spaced at least one inch from previous sites (WikiProjectMed 2024). Persistent use of the same spot creates localised lipoatrophy (fat loss) or lipohypertrophy (fat accumulation), both of which impair absorption. Keep a simple log of which site you used each session.
Mistake 6: Rushing the Withdrawal
Pulling the needle out immediately after the plunger bottoms out causes leakage of the injected fluid back through the needle track. Wait three to six seconds. This one pause, consistently applied, meaningfully improves tissue retention of the dose (Gradel 2016).
Mistake 7: Injecting into the Navel Zone
Stay at least two inches from the navel. The periumbilical tissue is denser, more vascular, and more sensitive. Injections too close to the navel are disproportionately painful and more likely to produce bruising (Brello Health 2026).
Pain Reduction Techniques
For most people using a 29–31 gauge needle, subcutaneous injection is nearly painless. The techniques that make the most measurable difference are: ensuring the alcohol prep pad is fully dry before injecting, inserting the bevel upward, and injecting slowly. A randomised controlled trial found that local vibration applied to the injection site reduced pain significantly compared to controls.
Practical pain reduction options in order of evidence quality:
- Bevel-up orientation: Point enters tissue first, reducing perceived sharpness (Great Ormond Street Hospital 2024).
- Dry alcohol site: Injecting into wet alcohol stings; 30 seconds drying time eliminates this.
- Slow injection: Rapid injection creates more pressure in the tissue depot.
- Local vibration: A small vibration device held adjacent to the injection site during administration reduced pain scores significantly in RCT data (p<0.001) (PMC 2024).
- Thigh vs abdomen: The upper thigh has fewer superficial nerve endings than the abdomen in some individuals; experiment with site preference.
Safe Sharps Disposal
Used syringes and needles must go directly into a rigid sharps container, never into the household bin, recycling, or down a drain. Improper sharps disposal creates needlestick risk for sanitation workers and household members. FDA-cleared sharps containers are inexpensive; most pharmacies also accept sealed containers for safe disposal.
The disposal protocol is simple:
- Do not recap the needle. Do not bend or break it. Place the used syringe directly into the sharps container immediately after withdrawal (Vaccine Allergy 2025).
- Use an FDA-cleared sharps container: rigid, puncture-resistant, leakproof, with a closeable lid. If an approved container is not available temporarily, a sturdy plastic bottle with a screw-on cap (laundry detergent jug, for example) labelled "SHARPS: DO NOT RECYCLE" is an acceptable interim solution (Vaccine Allergy 2025).
- When the container is three-quarters full, seal it and contact your local pharmacy, GP surgery, or council waste service for collection or drop-off options. Regulations vary by region; check locally.
- Keep the container out of reach of children and pets, and away from high-traffic areas.
WHO consensus data underscores that needle reuse and improper disposal are the two primary drivers of injection-related household injury in self-administering populations (PMC 2024). These are not bureaucratic formalities; they are the two safety behaviours that matter most outside the clinic.
Recognising and Responding to Injection-Site Reactions
Mild redness, a small raised welt, and minor itching at the injection site are common and usually represent a localised immune response to the needle puncture or to the benzyl alcohol in bacteriostatic water. These reactions typically resolve within one to two days and do not require medical attention. Signs that do require attention are different: increasing redness spreading outward, warmth, swelling, pain that worsens rather than improves over hours, or any pus formation.
Where to source it
Find research-grade peptides from vetted suppliers on our recommended sources page.
See the sources that passed →Distinguishing normal from concerning:
- Normal: Small red spot, mild itching, fades within 24–48 hours. Rotate sites, inject more slowly, ensure alcohol is fully dry before injection (Extension Health 2026).
- Concerning (seek medical attention): Redness spreading beyond 2 cm and enlarging over time, increasing warmth, pain worsening after 24 hours, swelling, or any discharge from the puncture site (Peptides Insider 2026).
The vast majority of injection-site reactions are minor and self-resolving. Proper technique, fresh needles, and systematic site rotation eliminate most of them entirely (Medical News Today 2026).
A Note on SubQ vs. Intramuscular for Peptides
Subcutaneous is the correct default route for virtually all peptide research protocols. It is safer, easier to self-administer, and works effectively for all major research peptides. Some compounds have specific intramuscular protocols in the research literature, but subcutaneous is the recommended starting route unless a specific compound protocol indicates otherwise.
If you are working with a specific compound and want route-specific guidance, the BPC-157 dosing and injection frequency guide provides a worked example of how SubQ frequency and dose selection interact in practice.
Building a Consistent Protocol: Practical Summary
Consistency is the variable that separates researchers who get results from those who do not. Syringe maths errors, missed doses from disorganisation, and injection-site complications from skipped rotation all introduce noise into any protocol. A written log, a fixed time of day, and a pre-laid supply kit eliminate most of the friction that breaks consistency.
A practical home setup:
- Keep your peptide vials refrigerated at 2–8°C, upright, sealed, away from light. Label every vial with the reconstitution date.
- Store syringes, alcohol prep pads, and sharps container together in one location so preparation is automatic.
- Log each injection: date, compound, dose in units, site used. A notes app on your phone is sufficient.
- Order a new supply of syringes before you run low. Running out mid-protocol and improvising is how reuse mistakes happen.
Always work with a qualified clinician before making changes to your health protocol. The dosing calculator handles the maths; your clinician handles the decision-making.
References
- Gradel AKJ et al. (2016). Injection technique and pen needle design affect leakage from skin after subcutaneous injections. PubMed 26798083
- MedlinePlus (2024). Subcutaneous (SQ) injections. medlineplus.gov
- FDA Clinical Trial Protocol NCT05275010 (2024). Pertuzumab-trastuzumab subcutaneous administration. clinicaltrials.gov
- PMC (2024). Effect of vibration on pain during subcutaneous heparin injection. PMC12596870
- Koivisto VA, Felig P (1992). The abdomen, thigh, and arm as sites for subcutaneous injections. PubMed 1857645
- PMC (2014). Injection device-related risk management toward safe administration. PMC3962321
- PMC (2024). Access, awareness, and risk: drivers of unsafe sharps disposal and needle reuse. PMC12657182
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.
Share this article
Frequently Asked Questions
What angle should I use for subcutaneous injection?
What is the difference between syringe units and International Units (IU)?
How do I convert my peptide dose into syringe units?
Why is injection site rotation essential?
Can I reuse insulin syringes to save money?
How long is a reconstituted peptide stable, and how do I store it?
Want our research first on Google? Add Underground Biohacking as a preferred source. Takes 10 seconds, one click to undo.
Read Next

Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.