
Retatrutide vs Tirzepatide vs Semaglutide: The Evidence Compared


Retatrutide vs Tirzepatide vs Semaglutide: The Core Difference
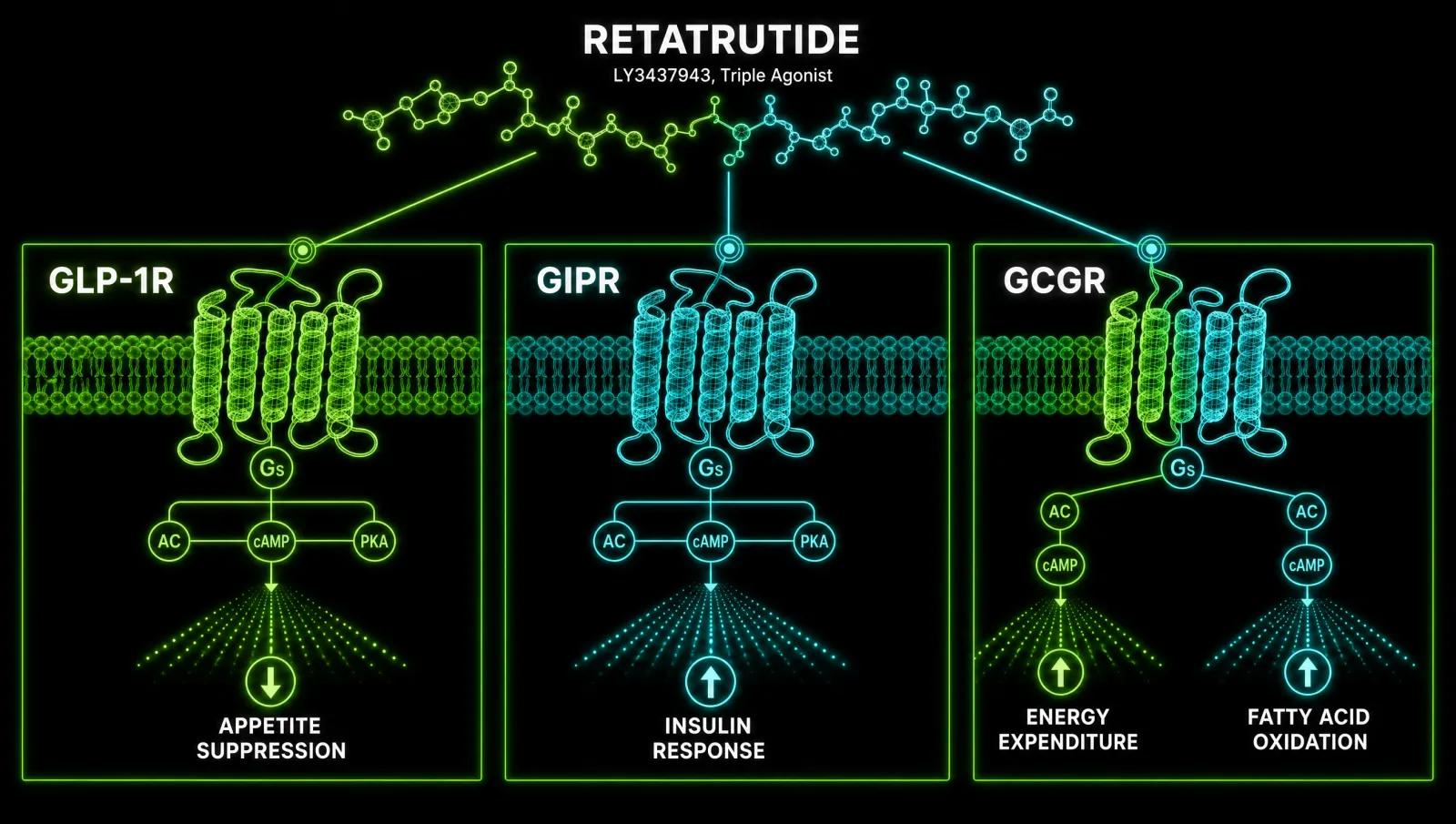
Retatrutide vs tirzepatide comes down to receptor count. Tirzepatide activates two hormone receptors (GIP and GLP-1), while retatrutide adds a third, the glucagon receptor. Semaglutide activates only one, GLP-1. More receptors generally means stronger weight loss, but a wider side effect profile you need to weigh carefully before deciding.
Both GIP and GLP-1 work on the brain's satiety circuits to reduce food intake, but they aren't identical twins. GLP-1 suppresses glucagon and slows gastric emptying, while GIP has the opposite glucagonotropic effect during low blood sugar, meaning the two receptors act as a balancing pair rather than a simple additive stack. Liu 2024 lays out this mechanism clearly, and it's the reason dual agonism (tirzepatide) doesn't just double GLP-1's effect, it changes how the body responds to it.
Retatrutide's third target, the glucagon receptor, is where things get genuinely different. Glucagon receptor activation increases energy expenditure rather than just suppressing appetite, which is a distinct lever that neither semaglutide nor tirzepatide pulls. Katsi 2025 frames this triple-receptor design as the reason retatrutide has outperformed dual agonists in preclinical models, not because it's simply "more of the same drug" but because it's working a different metabolic pathway on top of the shared one.
How the Trial Data Actually Stacks Up
Across separate Phase 2 and Phase 3 trials, retatrutide has produced the largest average weight loss, tirzepatide the most established and durable result, and semaglutide the longest real-world track record. None of these trials pitted all three head-to-head in the same population, so the numbers below are a guide, not a direct contest.
| Compound | Receptor targets | Trial result | Duration |
|---|---|---|---|
| Retatrutide | GIP + GLP-1 + glucagon | Up to 24.2% weight loss (12 mg) | 48 weeks, Phase 2 |
| Tirzepatide | GIP + GLP-1 | 22.5% weight loss (15 mg, efficacy estimand) | 72 weeks, Phase 3 |
| Semaglutide | GLP-1 only | 14.9% weight loss (2.4 mg) | 68 weeks, Phase 3 |
Retatrutide's Phase 3 data in type 2 diabetes showed a 15.3% mean body weight reduction at 40 weeks alongside a 1.94 point drop in HbA1c, with adverse events mostly mild to moderate gastrointestinal effects that eased over time, according to Bajaj 2026. Tirzepatide's registration trial found that its 15 mg dose delivered substantial, sustained weight reduction over 72 weeks, a result Jastreboff 2022 established as the benchmark that later reviews and meta-analyses, including a pooled analysis of nearly ten thousand patients by Lin 2023, confirmed as dose-dependent and consistent across studies.
Retatrutide itself was tested against active comparators in a US-based Phase 2 trial run by Rosenstock 2023, which is where much of the head-to-head confidence in retatrutide's ceiling effect comes from. Semaglutide's 14.9% figure, by contrast, comes from its own pivotal obesity trial run separately years earlier, so treat any single-number ranking as directional rather than a controlled shootout.
Liver Fat and Metabolic Effects Beyond the Scale
Weight loss on the scale doesn't tell you what's happening to visceral and liver fat, and this is where retatrutide has shown the most striking separation. A Phase 2a substudy in fatty liver disease found retatrutide reduced liver fat by an average that dwarfs what's been reported for either dual or mono-agonist therapy.
A body composition substudy in people with type 2 diabetes found that retatrutide preferentially reduces fat mass while preserving a greater proportion of lean mass than would be expected from weight loss of that scale, according to Coskun 2025. That distinction matters if you're an athlete or returning to competitive training after a layoff: losing fat without stripping the muscle you need to perform is a different outcome to a generic weight-loss result, even when the number on the scale looks similar.
Who Retatrutide Suits
Retatrutide suits someone chasing the outer edge of metabolic change, particularly fat loss combined with liver health, but it isn't something you can walk into a pharmacy and get. As of mid-2026 it remains investigational, meaning access runs through clinical trial enrolment rather than a prescription.
If your priority is maximum fat reduction and you're comfortable with an agent that has less real-world safety history and a transient heart rate signal at higher doses during early trials, retatrutide is the one to watch. It is not yet the practical choice for most people simply because it isn't broadly available.
Who Tirzepatide Suits
Tirzepatide suits the reader who wants the strongest weight loss currently available through a standard prescription pathway. It has the deepest Phase 3 evidence base of the three, a well-characterised safety profile, and it's already the compound most clinicians reach for when semaglutide plateaus.
It's a reasonable middle ground: meaningfully stronger than semaglutide on the scale, with a side effect profile that mirrors the GLP-1 class you're likely already familiar with. If you've stalled on semaglutide and want to escalate before considering something investigational, this is the logical next step.
Who Semaglutide Still Suits
Semaglutide still suits anyone who wants the longest-standing safety track record of the three or who responds well to a single-receptor approach without needing the extra efficacy of dual or triple agonism. It's the most studied in the real world, not just in trials.
For a reader newer to this drug class, or one who wants to start conservatively before considering a stronger agent, semaglutide remains a sensible entry point. The ceiling is lower, but the data behind it spans years of post-approval use across a huge population.
Safety Profile and Side Effects to Expect
All three share the same core side effect signature: nausea, diarrhoea, constipation and vomiting, almost always dose-dependent and easing over the first several weeks. Where they diverge is in the details, and retatrutide carries at least one signal the other two don't.
Tirzepatide's tolerability profile is well mapped: a review of the SURMOUNT program found it allows many people to reach or exceed 20% weight loss with a safety profile broadly similar to existing GLP-1 therapy, per Hamza 2025. Its durability trial found that stopping treatment led to substantial weight regain, which Aronne 2024 frames as evidence that these are chronic-use medications, not short courses.
Retatrutide's Phase 3 program showed discontinuation rates that climbed with dose, from roughly 4% at the lowest dose tested up to 11% at the highest, mostly driven by tolerability rather than serious adverse events, and its TRIUMPH program (evaluating 4, 9 and 12 mg weekly doses) is designed around that dose-escalation strategy according to Giblin 2026. This is the one area where retatrutide's added receptor comes with an added tolerability cost you should factor in.
Availability and Regulatory Status in 2026
Only tirzepatide and semaglutide are approved and prescribable for weight management right now. Retatrutide remains investigational, which means the only route to it is enrolment in an active clinical trial rather than a prescription from your GP or a compounding pharmacy.
That gap matters more than the efficacy numbers for most readers. A compound with a higher ceiling on paper is irrelevant if you can't legally access it, and the regulatory pathway for retatrutide is still working through the multi-indication basket trial structure covering obesity, sleep apnoea and knee osteoarthritis before any approval decision lands.
How to Decide Between Them
Decide based on what's actually available to you, not just the trial numbers. If you can access tirzepatide or semaglutide today, the decision is a real one between two approved options; if you're weighing retatrutide, the decision is really about whether trial enrolment fits your circumstances at all.
Whichever path you're considering, work with a qualified clinician before making any changes to your protocol, particularly given the dosing ranges involved (4 to 12 mg weekly for retatrutide, 5 to 15 mg for tirzepatide, 2.4 mg for semaglutide) and the fact that gastrointestinal tolerability is dose-dependent across all three. If you're researching how peptide-class compounds are sourced and verified more broadly, our guide on how to know if peptides are real covers the verification questions worth asking before you consider anything investigational. For a vendor-neutral overview of where researchers source compounds discussed on this site, see our recommended sources page.
Where to source it
If you're researching this compound, I've linked a trusted source below. It supports the channel.
See the sources that passed →References
- Liu. Mechanisms of action and therapeutic applications of GLP-1 and dual GIP/GLP-1 receptor agonists. 2024.
- Katsi et al. Retatrutide: A Game Changer in Obesity Pharmacotherapy. 2025.
- Bajaj et al. TRANSCEND-T2D-1 Phase 3 trial. 2026.
- Jastreboff et al. Tirzepatide Once Weekly for the Treatment of Obesity. 2022.
- Lin et al. Weight loss efficiency and safety of tirzepatide: A Systematic review. 2023.
- Rosenstock et al. Retatrutide Phase 2 trial conducted in the USA. 2023.
- Coskun et al. Effects of retatrutide on body composition in people with type 2 diabetes. 2025.
- Hamza et al. Tirzepatide for overweight and obesity management. 2025.
- Aronne et al. SURMOUNT-4 Randomized Clinical Trial. 2024.
- Giblin et al. TRIUMPH registrational clinical trials rationale and design. 2026.
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.
Where to source it
If you're researching this compound, I've linked a trusted source below. It supports the channel.
See the sources that passed →Share this article
Frequently Asked Questions
What is the difference between retatrutide, tirzepatide, and semaglutide?
Which one causes the most weight loss?
Are all three available right now?
What are the main side effects across the three?
What happens if I stop taking one of these medications?
How much liver fat reduction can these compounds achieve?
Read Next

Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.