
Retatrutide Dosage and Titration: What the Trials Actually Used


Retatrutide Dosage: What the Phase 2 Trials Actually Used
Retatrutide dosage in Phase 2 trials ran from 1 mg to 12 mg once-weekly via subcutaneous injection. The standard titration started at 2 mg, escalating every four weeks. At the 12 mg ceiling, participants lost an average of 24.2% of body weight over 48 weeks. (Jastreboff 2023)
Retatrutide (LY3437943) is not yet approved for clinical use. The dosing data below comes exclusively from published clinical trials. This article reports what trial investigators used and why. It does not constitute prescribing guidance.
For information on sourcing research peptides, see our recommended sources page.
Why Retatrutide Is Different From Other GLP-1 Drugs
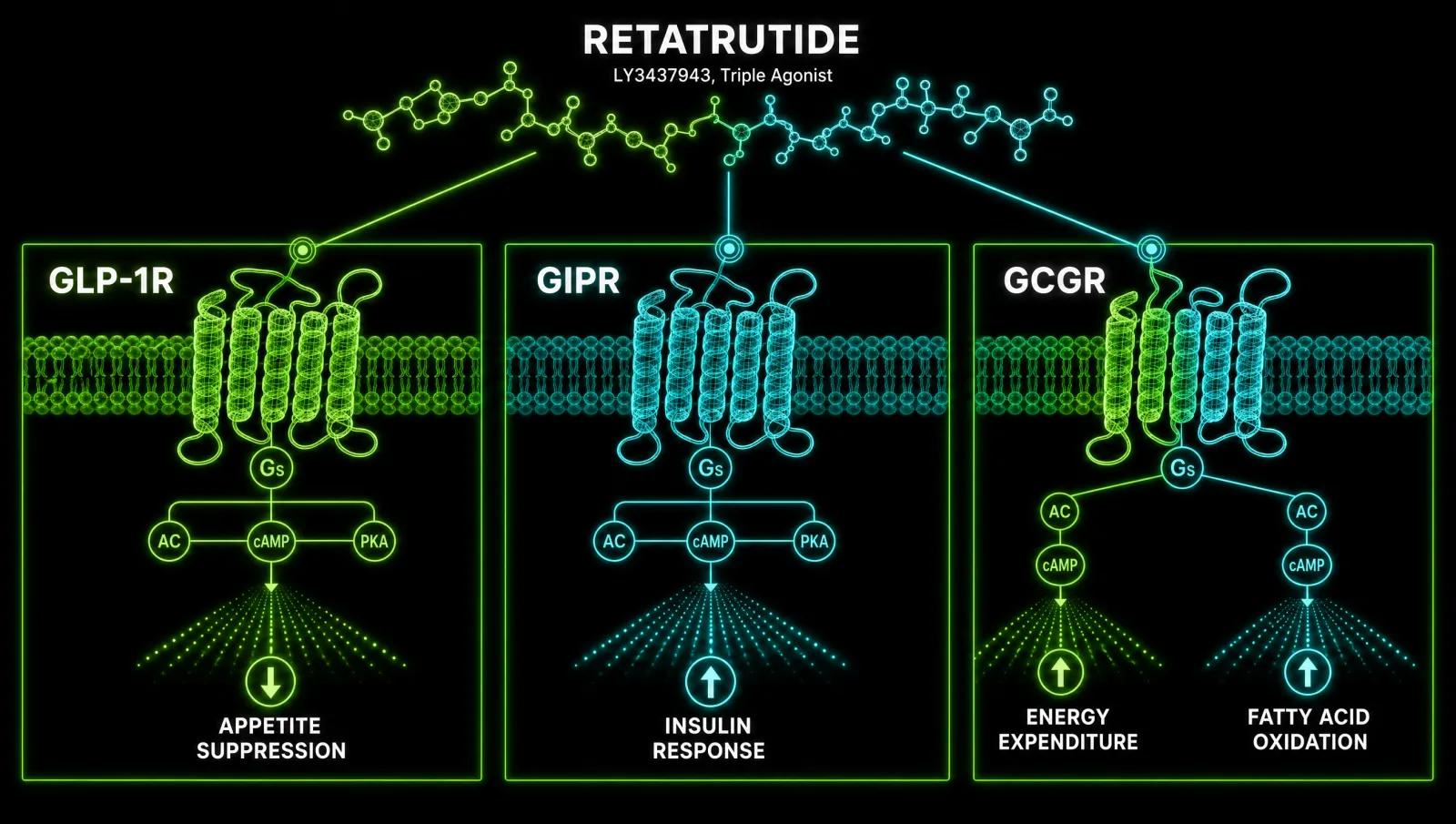
Retatrutide activates three receptors simultaneously: GLP-1R, GIPR, and GCGR. No approved obesity drug targets all three. This triple mechanism drives weight loss through appetite suppression, improved glucose and lipid metabolism, and increased energy expenditure via thermogenesis and lipolysis.
The pharmacological fingerprint matters for understanding its dosing logic. Retatrutide is a single synthetic peptide attached to a fatty diacid chain. Its receptor potency is deliberately imbalanced: it binds GIPR at 8.9 times the potency of endogenous GIP, yet binds GLP-1R at only 0.4 times and GCGR at only 0.3 times the endogenous ligands. (Katsi 2025)
That imbalance is intentional. High GIPR engagement enhances postprandial glucose control and synergises with GLP-1R-mediated appetite suppression, while the attenuated GCGR signal boosts energy expenditure without driving excessive hyperglycaemia. The net result is a metabolic intervention that outperforms dual agonists like tirzepatide in early head-to-model comparisons. (Doggrell 2023)
Phase 2 Trial Design: The Dose Ladder
The Phase 2 trial enrolled 338 adults with obesity or overweight, randomised to 1, 4, 8, or 12 mg once-weekly subcutaneous retatrutide or placebo for 48 weeks. Starting dose was 2 mg or 4 mg depending on cohort, with 4-week escalation steps between levels.
The randomised, double-blind, placebo-controlled design published in the New England Journal of Medicine in 2023 established the foundational dosing architecture still used by researchers and clinicians today. (Jastreboff 2023)
Key trial parameters:
- Route: subcutaneous injection (abdomen, thigh, or upper arm)
- Frequency: once weekly
- Maintenance doses evaluated: 1 mg, 4 mg, 8 mg, 12 mg
- Starting dose options: 2 mg (low-tolerability arm) or 4 mg (standard arm)
- Step interval: 4 weeks at each dose before escalation
- Trial duration: 48 weeks
The choice between a 2 mg and 4 mg start was not arbitrary. Investigators were testing a specific hypothesis about whether lower starting doses would reduce the gastrointestinal adverse event burden. The answer was definitive.
The 2 mg vs. 4 mg Start: Why It Matters for Tolerability
Starting retatrutide at 2 mg instead of 4 mg reduced nausea incidence from 60% to 17% in the 8 mg target-dose cohort. The lower start did not compromise weight loss at 48 weeks. Slow titration is not optional: it is the mechanism by which most patients reach and maintain higher doses.
This finding is one of the most clinically significant outputs of the entire Phase 2 programme. Gastrointestinal adverse events (nausea, diarrhoea, vomiting, constipation) are the primary tolerability challenge for all GLP-1-class drugs. Retatrutide is no exception. These events occur predominantly during dose escalation phases and diminish once a stable dose is maintained. (Jastreboff 2023)
The 2 mg starting dose gives the GI tract four weeks to adapt before the first escalation. The mechanism is thought to involve progressive receptor desensitisation and adaptation of gastric motility. Patients who forced through a 4 mg start were not experiencing worse long-term outcomes in terms of weight loss, but many discontinued earlier due to intolerable nausea during the escalation window.
For any researcher or clinician designing a protocol based on this trial, the 2 mg start is the data-supported default.
The Full Phase 2 Titration Schedule
The Phase 2 standard titration ladder was: 2 mg for 4 weeks, then 4 mg for 4 weeks, then 8 mg for 4 weeks, then 12 mg as the maintenance dose. Each step required four weeks at the current dose before escalation. No step could be skipped.
Expressed as a week-by-week schedule for those targeting the 12 mg ceiling:
- Weeks 1 to 4: 2 mg once weekly
- Weeks 5 to 8: 4 mg once weekly
- Weeks 9 to 12: 8 mg once weekly
- Week 13 onward: 12 mg once weekly (maintenance)
For participants targeting 4 mg or 8 mg maintenance, the ladder terminated at the target dose rather than continuing to 12 mg. The 1 mg arm used a single starting dose without a titration period, as it was below any escalation threshold.
Trial protocols explicitly allowed participants to pause escalation and remain at the current dose for an additional four-week period if gastrointestinal symptoms were significant. Dose reduction back to the last well-tolerated level was also permitted. Neither manoeuvre disqualified participants from the trial or appeared to compromise long-term weight loss outcomes. (Jastreboff 2023)
Phase 3 TRIUMPH Titration: What Changed
The Phase 3 TRIUMPH programme, enrolling over 5,800 participants, refined the titration ladder to: 2 mg, 4 mg, 6 mg, 9 mg, and 12 mg maintenance, each separated by 4-week intervals. The addition of a 6 mg intermediate step smooths the transition from the Phase 2 jump between 4 mg and 8 mg.
TRIUMPH-1 and TRIUMPH-2 target weight management outcomes over 68-week primary windows. TRIUMPH-3 and TRIUMPH-4 nest obstructive sleep apnoea and knee osteoarthritis outcomes within the same framework. Maintenance doses evaluated across the programme are 4 mg, 9 mg, and 12 mg. (Giblin 2025)
The Phase 3 TRIUMPH titration week-by-week schedule:
- Weeks 1 to 4: 2 mg once weekly
- Weeks 5 to 8: 4 mg once weekly
- Weeks 9 to 12: 6 mg once weekly
- Weeks 13 to 16: 9 mg once weekly
- Week 17 onward: 12 mg once weekly (maintenance)
This five-step ladder represents the most methodologically rigorous titration protocol published to date. The additional 6 mg intermediate step was almost certainly informed by tolerability data from the Phase 2 cohort, where the direct 4 mg to 8 mg escalation produced the highest rate of dose-interruption events.
Dose-Dependent Efficacy: What Each Dose Level Delivered
Retatrutide produces dose-dependent weight loss across all levels tested. The 12 mg dose delivered 24.2% mean weight reduction at 48 weeks. Critically, 4 mg delivered 17.1% and 8 mg delivered 22.8%, meaning meaningful fat loss does not require reaching the maximum dose.
Full weight loss data from the 48-week Phase 2 trial:
- 1 mg: mean weight loss of 8.7% from baseline
- 4 mg: mean weight loss of 17.1% from baseline
- 8 mg: mean weight loss of 22.8% from baseline
- 12 mg: mean weight loss of 24.2% from baseline
- Placebo: 2.1% weight change from baseline
(Jastreboff 2023, Tewari 2025)
The diminishing marginal return between 8 mg and 12 mg (22.8% vs. 24.2%, a 1.4 percentage point difference) is significant. Participants who cannot tolerate escalation beyond 8 mg are not being meaningfully disadvantaged in terms of primary weight loss outcomes compared to those who reach 12 mg. The decision to push to maximum dose should be driven by individual response and tolerability, not a belief that the ceiling dose is categorically superior.
A systematic review and meta-analysis published in 2025 pooling data from four randomised controlled trials confirmed the dose-dependent relationship and rated the evidence quality as high. (Tewari 2025)
Pharmacokinetics and the Logic of Once-Weekly Dosing
Retatrutide has a half-life of approximately 6 days, making once-weekly dosing pharmacologically rational. Steady-state concentrations are reached within 4 to 5 weeks at any given dose level, which is exactly why the titration protocol uses 4-week intervals before each escalation step.
This is not administrative convenience. The 4-week interval is calibrated to the pharmacokinetics. Escalating before steady state is established means the prescriber is not assessing the patient's response to the current dose but to a transient pharmacological state. The titration interval and the half-life are deliberately aligned. (Tetelbaun 2024)
Additional PK considerations relevant to dosing decisions:
- Half-life: approximately 144 to 165 hours (~6 days)
- Elimination: dose-proportional across the 1 to 12 mg range
- Steady state: achieved in 4 to 5 weeks at each dose
- Washout: after the final injection, significant drug concentrations persist for approximately 30 days
- Route: subcutaneous injection only; no oral formulation has been evaluated in humans
The washout period has implications for anyone considering interrupting a protocol. Unlike a short-acting drug where missed doses produce rapid loss of effect, retatrutide maintains meaningful plasma concentrations for four weeks after the last injection. A one-week interruption does not represent a pharmacological reset.
Reconstitution Maths for Research Applications
Retatrutide research vials typically contain lyophilised powder at 5 mg or 10 mg per vial. Adding 1 mL of bacteriostatic water to a 5 mg vial produces a 5 mg/mL concentration, where each 0.1 mL drawn into a 100-unit insulin syringe delivers 0.5 mg. Adjusting the volume drawn scales the dose proportionally.
Standard reconstitution reference table for a 5 mg vial with 1 mL bacteriostatic water (5 mg/mL):
- 2 mg dose: draw 0.40 mL (40 units on a 100U syringe)
- 4 mg dose: draw 0.80 mL (80 units on a 100U syringe)
- 5 mg dose: draw 1.00 mL (100 units on a 100U syringe, full vial)
For a 10 mg vial with 2 mL bacteriostatic water (also 5 mg/mL):
- 2 mg dose: draw 0.40 mL (40 units)
- 4 mg dose: draw 0.80 mL (80 units)
- 8 mg dose: draw 1.60 mL (160 units, requires a 2 mL syringe)
- 9 mg dose: draw 1.80 mL (180 units)
- 10 mg dose: draw 2.00 mL (full 10 mg vial in 2 mL)
For research use at 12 mg target doses, a 10 mg vial reconstituted in 1 mL bacteriostatic water (10 mg/mL) produces:
- 12 mg dose: 1.20 mL per injection (draws from two vials if using 1 mL syringes)
Reconstitution notes:
- Inject bacteriostatic water slowly down the side of the vial, not directly onto the powder
- Do not shake; swirl gently until the powder dissolves
- Store reconstituted solution refrigerated at 2 to 8 degrees Celsius
- Use within 28 days of reconstitution (bacteriostatic water allows multi-dose use)
- Discard if solution is cloudy or contains visible particles
Always work with a qualified clinician before making changes to your health protocol.
Liver Fat Outcomes: The MASLD Substudy Data
A Phase 2a substudy in 98 participants with metabolic-dysfunction-associated steatotic liver disease showed dose-dependent liver fat reductions of 42.9% at 1 mg up to 82.4% at 12 mg at 24 weeks. These reductions were substantially larger than the weight loss percentages at the same time points, suggesting hepatic fat is a preferential target.
Full liver fat reduction data at 24 weeks:
- 1 mg: 42.9% reduction in liver fat
- 4 mg: 57.0% reduction in liver fat
- 8 mg: 81.4% reduction in liver fat
- 12 mg: 82.4% reduction in liver fat
(Harrison 2024, Harrison 2024)
The GCGR agonism component is likely the primary driver of the hepatic fat effect. GCGR activation promotes hepatic fatty acid oxidation (beta-oxidation) and reduces de novo lipogenesis. The 8 mg dose achieves approximately the same liver fat reduction as 12 mg (81.4% vs. 82.4%), a plateau effect that mirrors, though precedes, the weight loss plateau between those doses.
Side Effect Profile and What the Data Shows About Management
Gastrointestinal adverse events are the dominant tolerability concern with retatrutide, occurring primarily during dose escalation. Nausea, diarrhoea, vomiting, and constipation are the most frequently reported. Slow titration and the 2 mg start are the primary evidence-based mitigation strategies available in the trial data.
The systematic review and meta-analysis confirmed that adverse events are dose-dependent and comparable to the broader GLP-1/GIP drug class. (Tewari 2025) The most clinically meaningful tolerability data point remains the 2 mg vs. 4 mg start comparison: 17% vs. 60% nausea incidence in the 8 mg target-dose cohort. (Jastreboff 2023)
Tolerability management options supported by trial protocols:
- Use the 2 mg starting dose regardless of target maintenance dose
- Maintain each dose for the full 4 weeks before any escalation attempt
- Pause escalation for an additional 4 weeks if GI symptoms are significant at the current dose
- Reduce back to the last well-tolerated dose if symptoms are severe
- Reattempt escalation after a period of dose stability
There is no evidence from published trials that forced rapid escalation improves long-term weight loss outcomes. The 48-week efficacy data represents a slow, methodical escalation. Deviating from that protocol by accelerating dose increases is unsupported by the published evidence base.
Where Retatrutide Sits in 2025 and 2026
Retatrutide is currently in Phase 3 TRIUMPH trials but has not received regulatory approval from any major agency as of mid-2026. The compound remains available only as a research peptide in non-clinical contexts. Phase 3 data readouts are expected in 2025 and 2026, with a potential NDA filing timeframe of late 2026 to 2027.
Where to source it
Research-grade retatrutide is available from verified suppliers. Always verify purity certificates before use.
See the sources that passed →The TRIUMPH programme spans four trials with a combined enrolment exceeding 5,800 participants across weight management, obstructive sleep apnoea, and knee osteoarthritis indications. (Giblin 2025) The breadth of the TRIUMPH programme reflects the confidence that Eli Lilly, the developer, has placed in retatrutide as a platform compound rather than a single-indication drug.
For researchers tracking the evidence base as it develops, the NEJM Phase 2 publication remains the primary dosing reference. The TRIUMPH Phase 3 publications, when available, will supersede the Phase 2 titration data as the foundation for any clinical protocol design.
For context on how retatrutide compares mechanistically to other GLP-1-class compounds currently being researched, see our overview of how peptide compound classes differ in receptor specificity and clinical application.
References
- Jastreboff AM, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity. N Engl J Med. 2023. doi:10.1056/NEJMoa2301972
- Tetelbaun L, et al. The First Triple Agonist for Antiobesity: Retatrutide. Cardiol Rev. 2024. PMID 39724554
- Harrison SA, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease. PMC. 2024. PMC11271400
- Giblin K, et al. Retatrutide for the treatment of obesity, obstructive sleep apnea and knee osteoarthritis: Rationale and design of the TRIUMPH registrational clinical trials. Diabetes Obes Metab. 2025. PMID 41090431
- Tewari J, et al. Efficacy and safety of triple hormone receptor agonist retatrutide for the management of obesity: a systematic review and meta-analysis. Expert Rev Clin Pharmacol. 2025. PMID 39817343
- Katsi V, et al. Retatrutide: A Game Changer in Obesity Pharmacotherapy. PMC. 2025. PMC12190491
- Doggrell SA. Is retatrutide (LY3437943), a GLP-1, GIP, and glucagon receptor agonist a step forward in the treatment of diabetes and obesity? Expert Opin Investig Drugs. 2023. PMID 37086147
- Harrison SA, et al. Triple hormone receptor agonist retatrutide for MASLD. Nature Medicine. 2024. doi:10.1038/s41591-024-03018-2
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.
Where to source it
Research-grade retatrutide is available from verified suppliers. Always verify purity certificates before use.
See the sources that passed →Share this article
Frequently Asked Questions
What is the starting dose of retatrutide in clinical trials?
How fast should retatrutide dose be increased?
What is the maximum dose of retatrutide tested in trials?
How long does retatrutide stay in your system?
Why does slow titration matter for retatrutide tolerability?
Do patients need to reach 12 mg to achieve meaningful weight loss with retatrutide?
Read Next
Retatrutide Explained: How the Triple Agonist Actually Works

AOD-9604 Dosage and Cycling: Injection Timing, Fasted Cardio Stack, and Maintenance (2026)

Tesamorelin Dosage Protocol: Daily Dosing, Fat-Loss Timing, and Cycle Length (2026 Guide)
Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.