
Retatrutide Explained: How the Triple Agonist Actually Works

What Is Retatrutide? The Triple Agonist Mechanism Explained
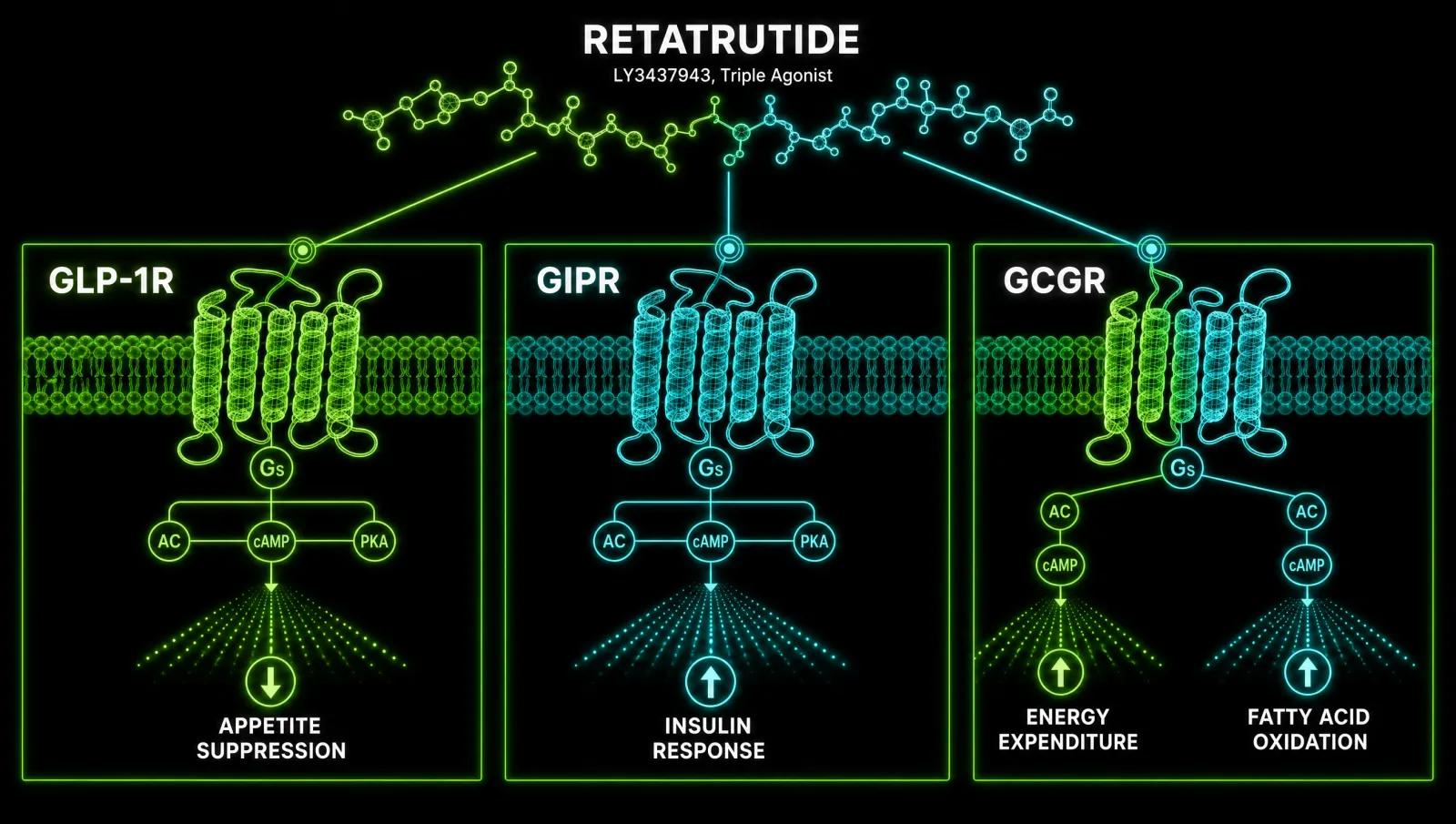
Retatrutide is a single-molecule triple agonist that simultaneously activates three hormone receptors: GLP-1 (glucagon-like peptide-1), GIP (glucose-dependent insulinotropic polypeptide), and glucagon. This triple-receptor strategy is what separates retatrutide from every approved weight-loss medication on the market today and explains why Phase 3 trial results are producing weight loss figures the pharmacology world has never seen in a drug.
Developed by Eli Lilly under the research designation LY3437943, retatrutide is currently investigational and undergoing Phase 3 clinical trials. It is not FDA-approved. But the mechanism behind it is worth understanding now, because it represents a genuine shift in how metabolic pharmacology targets the obesity problem, not just caloric regulation through one pathway, but three distinct and complementary hormonal axes firing simultaneously.
This article is a research-grounded explainer of that mechanism: how each receptor contributes, what the clinical trial data actually shows, how retatrutide compares to tirzepatide and semaglutide, and what the safety and regulatory picture looks like heading into 2027. All claims are sourced to primary literature.
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.
The Three Receptors: What Each One Does
Retatrutide's three target receptors each contribute a distinct metabolic function: GLP-1R reduces appetite and slows gastric emptying, GIPR enhances insulin secretion and glucose handling, and GCGR increases hepatic energy mobilisation and fatty acid oxidation. Targeting all three simultaneously is what drives the compound's superior weight loss profile over single and dual agonists.
To understand why a triple agonist outperforms its predecessors, you need to understand what each receptor pathway actually does.
GLP-1 Receptor (GLP-1R)
Glucagon-like peptide-1 receptors are expressed across multiple tissues: the pancreas, brain, gut, and cardiovascular system. GLP-1 signalling reduces appetite through central hypothalamic mechanisms, slows gastric emptying to reduce caloric absorption rate, and promotes glucose-dependent insulin secretion from pancreatic beta cells. GLP-1R and GIPR are class B G protein-coupled receptors (GPCRs) that signal through the Gαs-cAMP pathway, coupling hormone binding to downstream insulin secretion and cellular glucose uptake. Tanday 2024. Semaglutide (Wegovy, Ozempic) targets this receptor exclusively and achieves approximately 15% weight loss in trials.
GIP Receptor (GIPR)
Glucose-dependent insulinotropic polypeptide receptor signalling enhances the insulin secretory response to meals, improves peripheral glucose uptake, and appears to provide some protection against hypoglycaemia when GLP-1R is co-activated. GIP and GLP-1 play critical roles in biological processes across multiple tissues including the pancreas, fat, bone, and brain. Tanday 2024. Tirzepatide (Mounjaro, Zepbound) adds GIPR agonism to GLP-1R, producing approximately 22.5% weight loss.
Glucagon Receptor (GCGR)
This is the receptor that differentiates retatrutide from everything that came before it. Glucagon receptor activation facilitates hepatic glucose output and glycogenolysis and promotes fatty acid oxidation, contributing to the drug's superior weight loss profile. Piccini 2024. Crucially, this means retatrutide does not just suppress appetite. It actively increases energy expenditure at the metabolic level, a distinct mechanism that the GLP-1 and GIP arms cannot replicate. Animal data confirms this directly: retatrutide induces greater body weight losses in obese mice than tirzepatide, due to increased energy expenditure through GCGR activation. Piccini 2024
The structural basis for this triple activation has been characterised in molecular detail. A Nature-published study using molecular modelling and receptor-binding studies provided structural insights into retatrutide's simultaneous agonism at GLP-1R, GIPR, and GCGR, confirming that retatrutide binds all three as a single molecule without losing potency at any individual receptor. Du 2024
Phase 2 Trial Results: What the Early Data Showed
Phase 2 trials of retatrutide showed dose-dependent weight loss reaching 24.2% at 48 weeks with the 12 mg dose, a result that outperformed anything previously recorded for a pharmacological agent at that timepoint. These were randomised controlled trials, not observational data.
Phase 2 obesity trial data established retatrutide as the highest-performing weight-loss agent ever studied at that point in pharmaceutical development. A systematic review and meta-analysis of the available RCT data showed that retatrutide-treated participants achieved a mean body weight reduction of 10.66 kg and a BMI reduction of 4.53 kg/m², with significant proportions achieving weight loss thresholds of 5%, 10%, 15%, and 20% versus placebo. Deng 2024
The dose-response relationship was clear. At 24 weeks, participants on 12 mg retatrutide had lost 17.5% of body weight. By 48 weeks that figure reached 24.2%. Jastreboff 2024. A separate meta-analysis quantified the threshold data: the relative risk of achieving 5% weight loss was 2.92; for 10% it was 9.32; for 15% it was 18.40; and for 20% it was 16.61, all versus placebo. Deng 2024
These are not marginal effects. An 18-fold increase in the probability of losing 15% of body weight versus placebo is a pharmacological signal with bariatric surgery-magnitude implications.
Phase 3 TRIUMPH-1: The 28.3% Weight Loss Data
The Phase 3 TRIUMPH-1 trial, announced in May 2026, reported 28.3% average weight loss at the 12 mg dose over 80 weeks, approximately 71 pounds on average, with no weight loss plateau observed through week 80. This is the highest weight loss efficacy ever recorded for a pharmaceutical agent in a pivotal registrational trial.
The TRIUMPH program enrolled more than 5,800 participants across multiple registrational trials evaluating retatrutide across obesity, obstructive sleep apnoea, and knee osteoarthritis comorbidities. Wadden 2024. The basket design reflects the recognition that obesity does not exist in isolation: its comorbidities are the clinical problem, and a drug that can address body weight, liver fat, glycaemic control, and joint load simultaneously changes the calculus.
The key phrase in the TRIUMPH-1 announcement is that no weight loss plateau was observed through week 80. Lilly 2026. This is in contrast to the plateau patterns seen with semaglutide around weeks 60 to 65 in STEP trials. Whether continued GCGR-mediated energy expenditure explains the sustained trajectory is not yet formally characterised, but the mechanistic hypothesis is consistent with the animal data.
Phase 3 also included TRANSCEND-T2D-1, the first Phase 3 trial for type 2 diabetes. At 40 weeks, retatrutide achieved up to 2.0% A1C reduction alongside significant weight loss, again with no plateau observed. Lilly 2026
How Retatrutide Compares to Tirzepatide and Semaglutide
Head-to-head network meta-analysis data shows retatrutide produces greater absolute and percentage weight loss than tirzepatide: a mean difference of 16.34 kg absolute weight reduction and 23.77% percentage weight loss versus tirzepatide's 16.79%. Semaglutide, operating on GLP-1R alone, produces approximately 15% weight loss, roughly half retatrutide's Phase 3 efficacy.
A network meta-analysis comparing tirzepatide and retatrutide across clinical trial data found retatrutide superior efficacy in both absolute and percentage weight reduction. Comparative Network Meta-Analysis 2024. The key differentiator mechanistically is GCGR activation: tirzepatide has no glucagon component. Its dual GIP/GLP-1 mechanism targets appetite suppression and insulin response, but does not add the energy-expenditure dimension that retatrutide's glucagon arm provides.
The comparison table by mechanism:
- Semaglutide: GLP-1R only. Appetite suppression, gastric emptying, glucose-dependent insulin secretion. Phase 3 weight loss approximately 15%.
- Tirzepatide: GIP/GLP-1 dual agonist. Adds insulin response optimisation and some GIP-mediated glucose handling. Phase 3 weight loss approximately 22.5%.
- Retatrutide: GLP-1/GIP/GCGR triple agonist. Adds hepatic energy mobilisation, fatty acid oxidation, increased energy expenditure. Phase 3 weight loss 28.3%.
The caveat is clinical availability. Tirzepatide and semaglutide are FDA-approved and accessible through prescribers now. Retatrutide remains investigational, with NDA submission expected Q4 2026 and projected approval late 2027 or early 2028.
For a deeper look at how tirzepatide compares to semaglutide at the mechanism level, see our breakdown of how growth hormone secretagogues differ mechanistically, which applies similar receptor-level analysis to a related compound class.
Liver Fat and MASLD: The Phase 2a Substudy Data
A Phase 2a substudy in metabolic dysfunction-associated steatotic liver disease showed retatrutide 12 mg reduced liver fat by 82.4% at 24 weeks, with 86% of participants achieving normal liver fat levels below 5%. This is the most striking data point in the entire retatrutide dataset for secondary metabolic benefit.
The liver fat substudy data deserves its own discussion because metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD) is one of the largest unmet needs in metabolic medicine, and there are few approved pharmacological interventions. The Phase 2a randomised trial showed dose-dependent liver fat reduction: at 1 mg, liver fat fell 42.9%; at 4 mg, 57.0%; at 8 mg, 81.4%; and at 12 mg, 82.4% at 24 weeks. Gastaldelli 2024. At 12 mg, 86% of participants achieved normal liver fat, defined as below 5%, versus 0% in the placebo arm.
The mechanism here is multi-factorial: GLP-1R activation reduces hepatic lipogenesis, GIP receptor signalling improves peripheral fat handling, and GCGR activation promotes hepatic fatty acid oxidation directly. The combined effect on liver fat exceeds what any single or dual agonist has produced in comparable timeframes.
Safety Profile and Side Effects
Retatrutide's adverse event profile is dominated by gastrointestinal effects including nausea, vomiting, diarrhoea, and constipation, and these are dose-dependent and transient. Serious adverse events occurred at comparable rates to placebo in Phase 2 trials (4% in both arms). Gradual dose titration is the primary mitigation strategy and a critical component of the dosing protocol.
The gastrointestinal event pattern is consistent with the drug class and with the mechanism: GLP-1R-mediated slowing of gastric emptying produces nausea and early satiety, and this is most pronounced at the initiation and escalation phases. A key finding from trial data: participants who skipped titration experienced nearly double the GI symptom rates compared to those who followed the gradual escalation schedule. Deng 2024
The standard dose-escalation protocol observed in clinical trials: starting at 0.5 mg once weekly, then escalating through 1, 2, 4, 6, 8, 9, and 12 mg over approximately 20 weeks. Wadden 2024. The escalation schedule is not optional; it is a safety-critical design feature of the protocol.
A modest heart rate increase of up to 6.7 bpm was noted in Phase 2 data. Jastreboff 2023. This is consistent with observations in the GLP-1 drug class generally and is being monitored in the TRIUMPH cardiovascular outcomes programme. A meta-analysis of 4 RCTs confirmed the safety profile was comparable to control and that retatrutide was clinically and statistically superior to placebo on all primary weight loss endpoints. Systematic Review 2024
Regulatory Status and What Happens Next
Retatrutide is currently investigational and not FDA-approved. The TRIUMPH Phase 3 programme is ongoing, with NDA submission expected in Q4 2026 and approval projected for late 2027 or early 2028. It is not available for clinical prescribing.
The TRIUMPH programme is the most ambitious registrational basket in obesity pharmacology. More than 5,800 participants are enrolled across trials covering obesity, type 2 diabetes, obstructive sleep apnoea, and knee osteoarthritis. Wadden 2024. The breadth reflects Eli Lilly's strategy of establishing retatrutide not just as a weight-loss drug but as a cardiometabolic platform.
TRIUMPH-1 results announced May 2026 represent the first pivotal Phase 3 data. TRANSCEND-T2D-1 data for type 2 diabetes followed in March 2026. Lilly 2026. Additional trials in OSA and osteoarthritis are ongoing.
The practical implication for anyone tracking this space: retatrutide is not accessible through prescribers at this time. For those interested in the compound class and the underlying mechanisms, understanding the published evidence base now positions you to evaluate clinical options intelligently when they become available. For vetted research-grade suppliers of compounds currently under investigation, see our recommended sources page.
Why the Triple Mechanism Matters for Metabolic Research
The paradigm shift retatrutide represents is systems pharmacology applied to obesity: rather than targeting one hormonal axis and accepting ceiling effects, the triple agonist approach simultaneously attacks appetite, insulin sensitivity, and energy expenditure, and the clinical data suggests these effects are synergistic rather than additive.
The comprehensive review framing retatrutide as a paradigm shift in multi-hormonal pharmacotherapy captures the real significance. Arora 2024. For decades, obesity pharmacology was constrained by single-pathway thinking: block appetite here, improve insulin there. Each approach hit a ceiling because metabolic homeostasis is a multi-variable system. The body compensates around single-axis interventions.
A triple agonist removes the compensation routes simultaneously. GLP-1R activation reduces intake. GIPR activation optimises glucose handling so reduced intake doesn't trigger hypoglycaemic counter-regulation. GCGR activation increases output. The system's ability to maintain weight at a higher setpoint is disrupted from three directions at once.
Where to source it
Explore research-grade peptides and metabolic compounds from vetted suppliers on our recommended sources page.
See the sources that passed →This is why the comparison to bariatric surgery keeps appearing in the literature. Bariatric surgery produces weight loss in the 25 to 35% range through a combination of mechanical restriction and hormonal changes that are not fully characterised. Retatrutide at 28.3% in 80 weeks is producing pharmacologically what surgery produces anatomically, and doing so with a side-effect profile that serious adverse events comparable to placebo (4% in both arms).
Whether retatrutide changes long-term metabolic setpoints or requires indefinite administration to maintain effects is an open research question. The TRIUMPH programme's 80-week and beyond data will begin to address this. For now, the mechanism is the story, and the mechanism is genuinely novel.
References
- PMC12190491 - Retatrutide: A Game Changer in Obesity Pharmacotherapy (2025)
- PubMed 41545327 - Triple-Agonist Revolution: Retatrutide and the Paradigm Shift (2024)
- PMC11420505 - Meta-analysis of Retatrutide RCTs: Weight and Metabolic Markers (2024)
- Lilly TRIUMPH-1 - Phase 3 TRIUMPH-1 Results: 28.3% Weight Loss (2026)
- Lilly TRANSCEND-T2D-1 - Phase 3 Diabetes Trial Results (2026)
- Nature 2024 - Structural Insights into Triple Agonism at GLP-1R, GIPR, GCGR
- PMC11255275 - Triple Agonism: GLP-1R, GIPR, GCGR (2024)
- PMC12304053 - Triple Agonism Based Therapies for Obesity (2024)
- PubMed 38367045 - Retatrutide Phase II Clinical Trial Review (2024)
- PMC11304055 - Mechanisms of GLP-1 and Dual GIP/GLP-1 Receptor Agonists (2024)
- PMC11271400 - Retatrutide for MASLD: Phase 2a Liver Steatosis Trial (2024)
- PubMed 41090431 - TRIUMPH Phase 3 Trial Design (2024)
- PubMed 39817343 - Systematic Review and Meta-analysis: Retatrutide Efficacy and Safety (2024)
- PubMed 23947489 - Retatrutide Phase 2 Obesity and T2D (2023)
- PMC12544991 - Comparative Efficacy: Tirzepatide vs Retatrutide Network Meta-Analysis (2024)
- PMC12026077 - Retatrutide Systematic Review and Meta-analysis (2024)
This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.
Where to source it
Explore research-grade peptides and metabolic compounds from vetted suppliers on our recommended sources page.
See the sources that passed →Share this article
Frequently Asked Questions
What is retatrutide and how does it differ from other weight-loss medications?
How does retatrutide actually work in the body?
What weight loss results have been reported in clinical trials?
What are the main side effects of retatrutide?
Has retatrutide been FDA approved?
How does retatrutide compare to tirzepatide and semaglutide for weight loss?
Read Next


Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.