
Can Peptides Help Cure Loss of Smell? Evidence on Anosmia and Olfactory Repair (2026)
The Uncomfortable Truth About Peptides for Loss of Smell
Peptide advocates claim BPC-157, Semax, and TB-500 can reverse anosmia by flooding the olfactory epithelium with neurotrophins. The mechanism is real. The human evidence is not. Zero randomised controlled trials exist. Animal models do not replicate post-viral scarring. Clinical adoption has stalled for reasons the peptide community rarely discusses.
With BPC-157, the supplier matters as much as the dose. We only list sources that publish an independent, per-batch certificate of analysis. See the ones that clear it.
The Conventional Wisdom and Where It Goes Wrong
The standard peptide-community narrative runs as follows: the olfactory epithelium is uniquely capable of lifelong neurogenesis; peptides that upregulate nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF) should therefore accelerate olfactory neuron replacement; ergo, peptides can treat anosmia. This reasoning is not wrong exactly, but it skips over several inconvenient facts that explain why no regulatory agency has approved any peptide for smell loss, and why the handful of physicians experimenting in this space have not published replicable human data.
The problems begin with the biological prerequisites for peptide intervention to work. They are not trivially satisfied in the patients most desperate for treatment.
What the Olfactory Epithelium Actually Needs to Regenerate
The olfactory epithelium houses two stem cell populations with very different roles. Globose basal cells (GBCs) are the workhorse progenitors: they proliferate continuously, express the transcription factor cascade Sox2-Ascl1-Neurog1-NeuroD1, and produce new olfactory receptor neurons (ORNs) within days of mild-to-moderate injury. Horizontal basal cells (HBCs) are dormant sentinels that activate only after catastrophic epithelial damage and can regenerate the entire epithelial architecture including sustentacular cells, Bowman's gland cells, and GBCs themselves. Gadye 2017 (PMID 28479320)
This architecture matters because every peptide proposed for anosmia operates downstream of GBC survival. If GBCs are intact, the epithelium can regenerate and neurotrophic peptides may accelerate the timeline. If GBCs are destroyed by severe chemical injury, prolonged viral inflammation, or irradiation, the stem cell reservoir is gone. No neurotrophic signal, however potent, can direct differentiation from a progenitor pool that no longer exists. In those cases, respiratory metaplasia colonises the olfactory niche and the functional architecture is permanently replaced. Schwob 2013 (PMID 24361051)
Post-COVID anosmia typically preserves GBCs, which is why spontaneous partial recovery occurs in 60-80% of patients within 12 months without any intervention. The implication is underappreciated: in the cases where peptides have the best theoretical chance of working, the olfactory system is often already recovering on its own. The signal-to-noise problem for any clinical trial is severe.
The Neurotrophin Cascade: Real Biology, Overstated Clinical Implication
The mechanistic story that peptide proponents tell is built on genuine science. NGF binds TrkA receptors on newly born ORNs, supporting axon elongation toward the olfactory bulb. BDNF activates TrkB receptors, enhancing both ORN survival and neurogenesis within the olfactory bulb itself. Expression of both neurotrophins rises sharply in the olfactory epithelium 24-72 hours after epithelial injury, suggesting an endogenous repair signal. Buckland 1993 (PMID 8396736)
FGF-2 stimulates GBC proliferation directly. TGF-beta-2 biases progenitors toward neuronal rather than sustentacular fates. PDGF promotes survival of newly differentiated neurons before axon-target contact is established. This is a multi-step, temporally sequenced cascade, not a single switch. The problem with the peptide narrative is that it conflates "upregulates NGF/BDNF" with "completes the full regenerative sequence." A peptide that elevates BDNF systemically does not ensure that the elevated BDNF reaches the olfactory epithelium at the right concentration, at the right time, for the right duration, in the right cellular context.
This is not a minor caveat. It is the central reason clinical translation has failed.
Examining Each Peptide Candidate Against the Evidence Standard
Semax: The Strongest Mechanistic Case, the Weakest Clinical Data
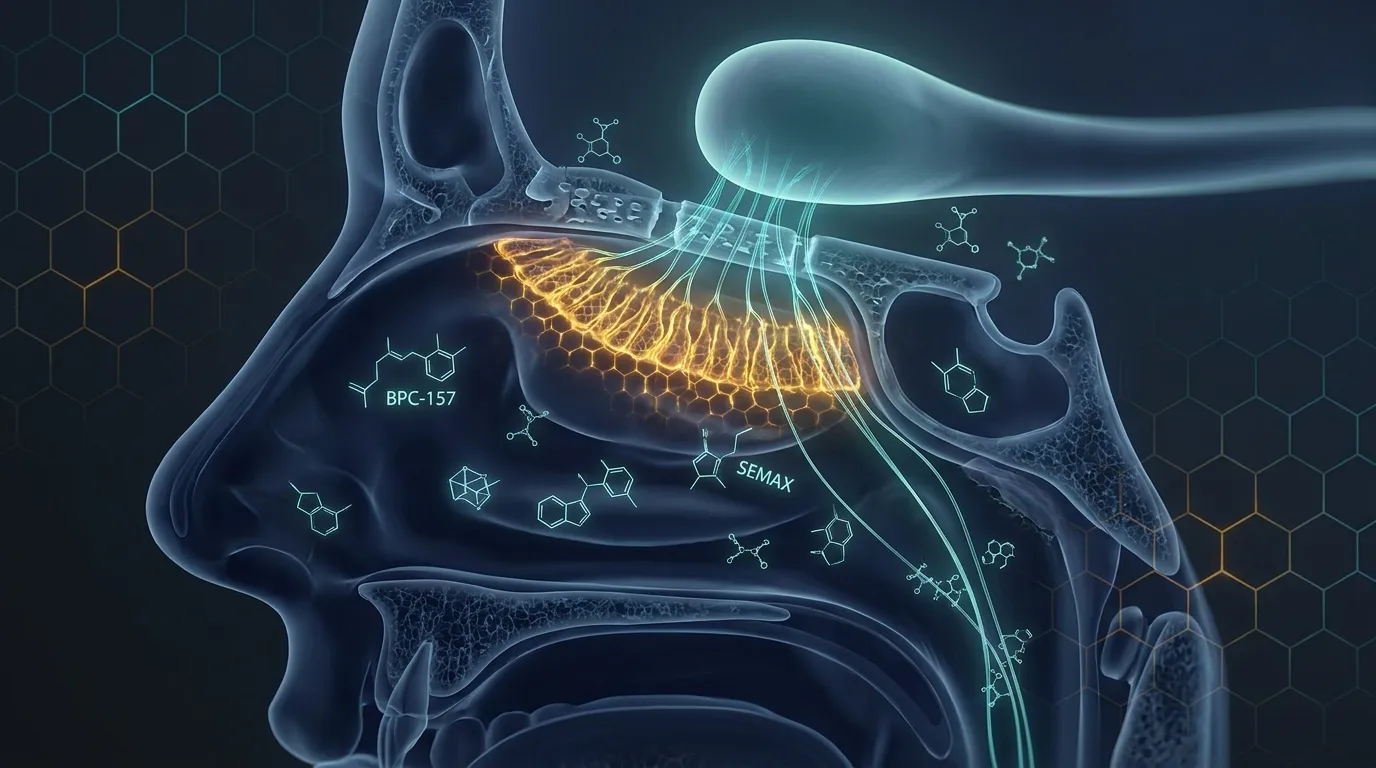
Semax is the ACTH(4-10) heptapeptide analogue with the most direct connection to olfactory neurotrophin biology. It was approved in Russia for stroke and optic nerve atrophy partly because intranasal delivery routes neurotrophic signals along the olfactory and trigeminal pathways directly into the CNS. Studies in rodents show BDNF and NGF mRNA upregulation in the hippocampus, basal forebrain, and olfactory structures within hours of a single intranasal dose. Dolotov 2006 (PMID 12203698)
The intranasal delivery argument is genuinely compelling. Compared with intravenous administration, intranasal Semax achieves roughly 9-fold better CNS penetration because the olfactory nerve provides an extraneuronal transport pathway bypassing the blood-brain barrier. This means the olfactory epithelium is simultaneously the delivery mechanism and the target tissue. If you are trying to get a neurotrophic signal to olfactory structures, intranasal is the correct route.
Where the narrative breaks down is at the clinical endpoint. Not a single published randomised trial has tested Semax specifically for anosmia in humans. The Russian clinical literature documents its use in optic atrophy and cognitive disorders, not smell loss. The mechanism is plausible; the efficacy is unproven. Anyone claiming Semax "treats anosmia" is extrapolating from neurotrophin pharmacology, not from clinical outcome data. You can read a fuller pharmacological breakdown in our Semax complete guide.
For educational purposes, research protocols in this space typically use 200-300 mcg per nostril targeting the superior turbinate twice daily, but this should only be pursued under guidance from a qualified clinician familiar with experimental peptide use.
BPC-157: Potent Angiogenic and Anti-inflammatory Effects, Zero Olfactory-Specific Data
BPC-157 (Body Protection Compound 157) is a 15-amino-acid peptide derived from a gastric cytoprotective protein sequence. Its most documented actions in preclinical models are angiogenesis via VEGF upregulation, reduction of inflammatory cytokines (TNF-alpha, IL-6), nitric oxide system modulation, and peripheral nerve repair acceleration. Sikiric 2000 (PMID 10604903)
The rationale for BPC-157 in anosmia rests on two observations. First, post-viral anosmia is partly mediated by sustained local inflammation in the olfactory mucosa, and BPC-157's anti-inflammatory profile might reduce the inflammatory microenvironment that suppresses GBC proliferation. Second, BPC-157 has demonstrated peripheral nerve regeneration in sciatic nerve crush models, accelerating functional recovery compared with controls. Staresinic 2006 (PMID 16639155)
Neither observation translates cleanly to olfactory repair. The olfactory epithelium is not peripheral nerve tissue. Its regenerative biology is governed by a stem cell cascade, not Schwann cell remyelination. The inflammatory pathways in post-COVID olfactory mucosa differ mechanistically from the gut and musculoskeletal inflammation where BPC-157 has been studied. No animal model of anosmia has been used to test BPC-157. The compound appears in anosmia discussions primarily because of its general pro-regenerative reputation, not because of any olfactory-specific mechanistic or empirical basis.
BPC-157 remains one of the most interesting experimental peptides in the repair space and is discussed extensively in our BPC-157 dosing protocol guide and our overview of best peptides for injury recovery, but its inclusion in anosmia protocols is currently speculative extrapolation.
TB-500 (Thymosin Beta-4): Genuine Corneal Data, Speculative Olfactory Extension
TB-500 is the synthetic fragment of Thymosin Beta-4 (TB4), a ubiquitous actin-sequestering protein with documented roles in wound healing, inflammation regulation, and tissue repair. Its most clinically relevant finding for any sensory application comes from corneal studies: topical TB4 accelerated corneal epithelial healing and neurite regrowth after injury in both animal models and a small human trial. Sosne 2002 (PMID 12220090)
The corneal data is cited by peptide advocates as evidence that TB-500 supports sensory neuron repair and therefore could help olfactory neurons. This is a category error. Corneal innervation is trigeminal, not olfactory. The cellular mechanisms of corneal epithelial repair are distinct from GBC-driven neurogenesis in the olfactory epithelium. The clinical precedent from corneal trials tells us TB4 can support trigeminal sensory recovery in one tissue, not that it activates the Sox2-Ascl1 transcription factor cascade required for olfactory neurogenesis.
TB-500 is detailed more thoroughly in our TB-500 complete guide for those interested in its documented applications.
Selank: Anxiolytic Properties, No Repair Mechanism
Selank is a heptapeptide analogue of tuftsin with well-documented anxiolytic and mild nootropic effects mediated partly through enkephalin degradation inhibition and GABA-A modulation. It appears in some anosmia discussions because anxiety and depression are frequent comorbidities of chronic smell loss, and because like Semax it is delivered intranasally.
There is no mechanistic pathway by which Selank's pharmacology supports olfactory neuron regeneration. It does not meaningfully upregulate neurotrophins relevant to olfactory repair, does not modulate the GBC stem cell cascade, and has not been tested in any olfactory injury model. Its inclusion in anosmia stacks appears to be pattern-matching from intranasal delivery and the Semax association rather than any independent mechanistic rationale. Contrast the two compounds in our Semax vs Selank comparison.
GHK-Cu: Anti-inflammatory and Angiogenic, Mechanism Misapplied
GHK-Cu (copper peptide) has documented effects on fibroblast proliferation, collagen synthesis, angiogenesis, and anti-inflammatory gene expression. In wound healing contexts it accelerates tissue remodelling and reduces scarring. The theoretical argument for anosmia is that it could reduce the fibrotic microenvironment around the cribriform plate that blocks regenerating ORN axons from reaching the olfactory bulb in post-traumatic cases.
This is the most defensible mechanistic extension in the anosmia peptide toolkit, but it remains entirely speculative. Cribriform plate fibrosis is a structural obstruction. Local intranasal delivery of GHK-Cu would need to reach periosteal tissue, modulate scar remodelling over weeks to months, and do so without disrupting the delicate olfactory epithelial architecture above. No model has demonstrated this. Our GHK-Cu complete guide covers its documented applications in more detail.
Why Clinical Adoption Has Stalled: The Real Reasons
If the mechanisms are real and the need is obvious, why has no major academic medical centre launched a peptide trial for anosmia? The stalling reflects several structural problems that the peptide community rarely acknowledges directly.
Regulatory Status Creates Trial Barriers
Most peptides relevant to anosmia, including Semax, BPC-157, and TB-500, exist in a regulatory grey zone in Western markets. The FDA's 2020 guidance on compounded peptides restricted their availability, and while some pathways remain open, conducting a formal IND (Investigational New Drug) application for a compound with no pharmaceutical sponsor, no patent protection, and no commercial return is extremely difficult. Academic researchers cannot easily run trials on compounds they cannot reliably source to pharmaceutical-grade purity. The regulatory environment is shifting, as covered in our FDA reclassification explainer, but the structural disincentive for peptide anosmia trials has been severe.
Spontaneous Recovery Confounds Interpretation
Post-COVID anosmia recovers spontaneously in the majority of patients within 12 months. Any uncontrolled case series or anecdotal report of peptide-treated anosmia will be heavily contaminated by spontaneous recovery. Without a randomised placebo arm, it is impossible to attribute recovery to the peptide rather than natural history. This is not a minor statistical footnote; it means every positive anecdote in the peptide community is essentially uninterpretable as evidence of efficacy.
Outcome Measurement Is Non-trivial
Validated olfactory testing requires Sniffin' Sticks, University of Pennsylvania Smell Identification Test (UPSIT), or butanol threshold testing conducted by trained examiners. Subjective patient reports of smell improvement correlate poorly with objective psychophysical measures. Most peptide case reports rely on patient self-report, which introduces enormous placebo and expectation bias given how motivated anosmia patients typically are.
Route of Administration Is Technically Demanding
For any neurotrophin-targeting peptide to reach the olfactory epithelium at therapeutic concentrations, it must be delivered intranasally to the superior turbinate, not simply squirted into the anterior nasal passage where it contacts respiratory mucosa rather than olfactory epithelium. Superior turbinate deposition requires device designs and delivery techniques that most patients and even most clinicians are not familiar with. Poor delivery technique means most intranasally administered peptide never reaches the target tissue, making the intervention pharmacologically inert regardless of the compound's intrinsic activity.
The One Clinical Analogue That Suggests Caution
The closest clinical analogue to peptide-for-anosmia is platelet-rich plasma (PRP) administered submucosally at the olfactory cleft. PRP concentrates multiple growth factors including PDGF, TGF-beta, VEGF, and EGF, delivering a broader spectrum of trophic signals than any single peptide. A 2021 pilot randomised trial by Yan et al. showed modest improvement in Sniffin' Sticks scores at 12 weeks compared with placebo injection in post-infectious anosmia patients with intact GBC populations on biopsy. Effect sizes were small and the trial was underpowered.
What does this tell us about peptides? First, even a multi-growth-factor cocktail delivered directly to the target tissue produces modest and variable results. Single-peptide interventions delivered via general intranasal spray face even steeper pharmacokinetic challenges. Second, patient selection matters enormously: only patients with biopsy-confirmed GBC preservation responded. Third, the effect required 12 weeks to manifest, suggesting that any peptide trial shorter than 3 months is probably underpowered to detect a real signal even if one exists.
Where the Evidence Genuinely Supports Optimism (Narrowly)
The pessimistic framing above should not be read as dismissing peptide intervention entirely. There is a narrow window where the mechanistic logic is tight and the population is well-selected. That window looks like this:
| Anosmia Type | GBC Status | Peptide Rationale | Evidence Quality |
|---|---|---|---|
| Post-COVID (early, under 6 months) | Usually intact | Moderate: Semax neurotrophin upregulation may accelerate GBC-driven recovery | Preclinical only |
| Post-COVID (chronic, over 12 months) | Variable: may have partial metaplasia | Low: metaplastic areas cannot respond to neurotrophins | Preclinical only |
| Post-infectious (non-COVID viral) | Usually intact | Moderate: similar rationale to early post-COVID | Preclinical only |
| Post-traumatic | Often intact but axon path obstructed | Very low: physical obstruction at cribriform plate limits value of neurotrophins | Theoretical |
| Congenital (Kallmann syndrome) | Absent or structurally deficient | None: developmental deficit not amenable to neurotrophin support | No basis |
| Toxic/chemical injury | Variable: severe cases lose HBCs and GBCs | Low to moderate depending on injury severity | Animal models only |
The honest summary is that Semax via superior turbinate delivery in confirmed post-viral anosmia with intact GBC populations (confirmed by biopsy or inferred from short duration and MRI evidence of olfactory bulb volume preservation) has the most defensible mechanistic rationale of any peptide intervention. That rationale is still preclinical. The other peptides have increasingly attenuated mechanistic justifications.
Comparing Peptides Against Established Interventions
| Intervention | Mechanism | Evidence Level | Effect Size (Human) | Availability |
|---|---|---|---|---|
| Olfactory training | Activity-dependent neuroplasticity, promotes ORN survival and bulb reorganisation | Multiple RCTs | Modest, consistent | Widely available, low cost |
| Intranasal corticosteroids | Reduces inflammatory obstruction of olfactory cleft | RCTs | Modest, mainly in inflammatory anosmia | Prescription, widely available |
| PRP submucosal injection | Multi-growth-factor trophic support at olfactory cleft | Small pilot RCTs | Small, variable | Specialist centres only |
| Vitamin A intranasal drops | Supports epithelial differentiation and ORN maturation | Retrospective series | Small signals in case series | Specialist compounding pharmacies |
| Semax intranasal | NGF/BDNF upregulation via olfactory delivery pathway | Preclinical + mechanism-inferred | Unknown in humans | Research peptide suppliers |
| BPC-157 intranasal | Anti-inflammatory, angiogenic; no olfactory-specific data | Preclinical (non-olfactory) | Unknown in humans | Research peptide suppliers |
| TB-500 systemic | Actin modulation, anti-inflammatory; corneal nerve precedent only | Preclinical + one small human trial (corneal) | Unknown for anosmia | Research peptide suppliers |
Olfactory training remains the only intervention with multiple randomised trials, replicable effect sizes, and a mechanistic explanation grounded in activity-dependent neuroplasticity research. Any peptide intervention, if pursued, should be combined with olfactory training rather than substituted for it. The combination logic is sound: olfactory training increases ORN activity and may upregulate endogenous neurotrophin expression, potentially amplifying the effect of exogenous neurotrophin support from peptides.
The Dosing and Delivery Reality Check
For those who have read the evidence above and still want to explore peptide intervention for research use, the pharmacokinetic constraints are non-negotiable regardless of which compound is chosen.
Superior turbinate targeting is essential. The olfactory epithelium covers the superior turbinate and the opposing portion of the nasal septum. Standard nasal sprays deposit over 90% of their dose in the anterior nasal passage below the olfactory cleft. Devices designed to deliver to the upper nasal vault, including certain breath-powered bidirectional devices and angled-nozzle sprays, are required for any meaningful olfactory epithelium contact. This is not optional; it is the pharmacokinetic prerequisite.
Concentration matters more than volume. The olfactory epithelial surface area accessible to topical delivery is small. High-concentration, low-volume delivery is preferable to large-volume irrigation. Standard 100 mcl spray volumes with concentrations of 200-500 mcg/ml for Semax represent the upper end of what has been discussed in research contexts.
Oral peptides are inert for this application. Gastric pH 1.5-3.5 hydrolyses peptide bonds before any systemic absorption occurs. Oral BPC-157 may have local gut effects through a different mechanism (see our BPC-157 gut health overview), but it cannot deliver intact peptide to the olfactory epithelium. Claims of oral peptide efficacy for anosmia lack pharmacokinetic plausibility.
Duration of at least 12 weeks is required to observe any signal. Olfactory neurogenesis from GBC to mature ORN with olfactory bulb axon contact takes 4-6 weeks in rodents and likely longer in humans. Trials or personal experiments shorter than 3 months cannot generate interpretable data.
This content is provided for educational purposes only. Peptides discussed here are research use compounds not approved by any regulatory agency for anosmia treatment. Anyone considering these interventions should work with a qualified clinician experienced in experimental peptide medicine who can assess individual suitability, monitor outcomes with validated psychophysical testing, and discontinue if adverse effects arise.
Where to source it
The hard part with BPC-157 isn't the protocol. It's finding a supplier that can prove what's in the vial. We assessed dozens against per-batch, third-party testing. A handful passed.
See the sources that passed →With BPC-157, the supplier matters as much as the dose. We only list sources that publish an independent, per-batch certificate of analysis. See the ones that clear it.
What a Meaningful Trial Would Actually Need to Show
The peptide-for-anosmia field is stuck in a cycle of plausible mechanisms and anecdotal reports. Breaking out of that cycle requires understanding what a meaningful clinical signal would look like. It is not a patient reporting "I can smell coffee again." It is:
- Randomised allocation with placebo arm using identical delivery device and protocol
- Stratification by aetiology (post-viral vs post-traumatic vs toxic) and GBC status on biopsy or surrogate measure
- Primary endpoint of change in Sniffin' Sticks TDI score (threshold, discrimination, identification) at 12 and 24 weeks
- Secondary endpoints including olfactory bulb volume on MRI and quality of life measures (SQOL-7 or equivalent)
- Intent-to-treat analysis accounting for the high rate of spontaneous recovery in the control arm
- Sample size calculated from the known spontaneous recovery rate (approximately 60% partial recovery at 12 months) to detect an additional peptide-attributable effect
No such trial exists for any peptide. Until it does, claims of efficacy remain at the level of mechanistic hypothesis, not clinical evidence. The mechanistic hypothesis is interesting enough to justify the trial being run. It is not sufficient to justify the certainty with which some peptide advocates recommend these compounds to desperate anosmia patients.
The Bottom Line: Mechanism Is Not Evidence
The peptide-for-anosmia argument is built on genuine and interesting biology. The olfactory epithelium does regenerate. Neurotrophins do support that regeneration. Semax does upregulate NGF and BDNF via the same intranasal route that targets olfactory tissue. BPC-157 does reduce inflammation in preclinical models. TB-500 did accelerate corneal sensory recovery in one small human trial.
None of that is the same as demonstrating that these compounds improve human olfactory function in a controlled setting. The leap from plausible mechanism to clinical recommendation is large, and the peptide community has been making it without the evidence to support the landing. The reasons clinical adoption has stalled are structural, not conspiratorial: regulatory barriers to trials on unpatentable compounds, a high spontaneous recovery rate that makes placebo-controlled trials necessary but expensive, and technically demanding delivery requirements that most clinical settings are not equipped to meet.
If you have anosmia, the evidence-based first steps remain olfactory training (rose, eucalyptus, lemon, clove for 20 seconds twice daily for at least 3 months) and intranasal corticosteroids if there is an inflammatory component. If you are interested in experimental peptide augmentation, Semax delivered properly to the superior turbinate is the candidate with the most internally coherent mechanistic rationale, and it should be explored only with a qualified clinician running proper outcome measurement, not based on forum anecdotes. The biology is compelling. The clinical evidence is not yet there. Those are both true simultaneously, and pretending otherwise helps no one.
Frequently Asked Questions
Where to source it
The hard part with BPC-157 isn't the protocol. It's finding a supplier that can prove what's in the vial. We assessed dozens against per-batch, third-party testing. A handful passed.
See the sources that passed →Share this article
Frequently Asked Questions
Can peptides actually restore sense of smell after COVID?
Which peptide is most likely to help with anosmia based on current evidence?
Why haven't researchers run clinical trials of peptides for smell loss?
Does BPC-157 help with loss of smell?
Does taking peptides orally work for anosmia?
How long would a peptide protocol for anosmia need to run to see results?
Want our research first on Google? Add Underground Biohacking as a preferred source. Takes 10 seconds, one click to undo.
Read Next

Disclaimer: This content is for educational purposes only. These compounds are intended for research use. Nothing here is medical advice. Always work with a qualified clinician before making changes to your health protocol.